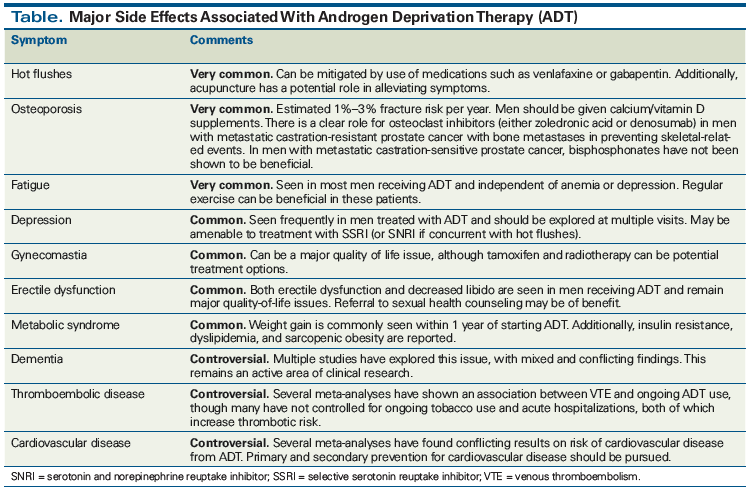
The standard treatment for men with metastatic prostate cancer is androgen deprivation therapy (ADT). This therapy is associated with a multitude of side effects that can impact quality of life. These include vasomotor complications (in particular, hot flushes), sexual dysfunction and gynecomastia, osteoporosis, metabolic syndrome, and depression. Additionally, ADT has been associated with neurocognitive deficits, thromboembolic disease, and cardiovascular disease, although the data regarding the latter associations are mixed. This article summarizes the key side effects associated with ADT and discusses strategies to optimize management.
Introduction
Metastatic prostate cancer remains a global health challenge. Despite improvements in anticancer therapies, management of the disease is often a struggle to maintain a balance between preserving quality of life and extending survival. Charles Huggins and Andrew Schally laid the groundwork for establishing the critical role of antiandrogen therapies in the management of metastatic prostate cancer.[1] Initially, androgen deprivation therapy (ADT) was achieved via orchiectomy, but by the mid-1980s, the approval of gonadotropin-releasing hormone (GnRH) agonists allowed for medical ADT.[2] Intermittent ADT represents an option for patients with biochemically relapsed prostate cancer, but continuous ADT is the standard initial treatment for metastatic disease. While prolonged disease control can be achieved with this approach, use of ADT is associated with a wide range of side effects (Table) that may significantly reduce quality of life. In this article, we summarize the key side effects associated with ADT and highlight strategies to mitigate them.
Vasomotor Complications
Hot flushes are one of the most common and bothersome side effects associated with ADT. Up to 80% of patients undergoing treatment with GnRH agonists will experience hot flushes, with 27% of these patients reporting this symptom as the most significant adverse side effect.[3] Hot flushes are described as an intense feeling of warmth, occasionally associated with nausea and night sweats. Many patients will achieve some improvement in symptom severity as their bodies acclimate to the low testosterone state, although some patients will not acclimate. Therapeutic management is largely extrapolated from studies in breast cancer patients receiving tamoxifen.[4] Randomized clinical trials have demonstrated efficacy of gabapentin and venlafaxine; these agents may be used for this off-label indication in men receiving ADT.[5,6] Low-dose estrogen and progestins can also be considered,[5] but the benefits of this option need to be weighed against the thromboembolic risk associated with estrogen use.[7] Additionally, acupuncture has been shown to be of potential benefit.[8] Conservative strategies to abort hot flushes include sleeping with an open window or drinking cold beverages. Lastly, regular exercise can help decrease frequency and severity of hot flushes; given the benefit of exercise for other ADT side effects and overall health, this recommendation is strongly encouraged. Overall, a stepwise approach is suggested for hot flush management, including exercise, conservative measures, use of venlafaxine or gabapentin, and lastly use of estrogen or progestins as needed, while weighing the potential risks vs benefits of each treatment option.
Sexual Dysfunction and Gynecomastia
Several studies have shown that treatment for clinically localized prostate cancer involving either radical prostatectomy, brachytherapy, or external beam radiotherapy (EBRT) can result in long-term erectile dysfunction.[9,10] Patients receiving neoadjuvant ADT with EBRT were found to have decreased frequency of erection, decreased overall sexual function, and an increase in frequency of hot flushes.[11] In addition, loss of libido is a major consequence of ADT. The degree of erectile dysfunction for patients on ADT is impacted by pretreatment sexual function, as well as by changes in libido; in patients previously able to attain an erection, phosphodiesterase 5 inhibitors, intracavernosal injection therapy, vacuum-assisted devices, or other topical agents may be used. Given the complex interplay between physiology, psychology, stress, and emotion involved in sexual function, a referral to a psychology or counseling service with a focus on sexual health is recommended for interested patients and their partners.
Gynecomastia may arise in conditions of unopposed estrogen activity and can be distressing for cosmetic reasons or because of pain. It may occur with ADT; however, it is more problematic with antiandrogens (specifically at higher doses) due to the buildup of androgens and their consequent peripheral conversion to estrogen in breast tissue. Tamoxifen and breast irradiation are two treatment options; the former is more beneficial as primary prevention, whereas the latter may be of greater use following established gynecomastia.[12,13]
Bone Health
ADT is associated with significant changes in bone. Multiple studies have demonstrated that bone mineral density (BMD) is significantly reduced in men receiving ADT compared with controls.[14] The risk of fracture increases with use of ADT and appears to be dose dependent.[15] Prevention of skeletal-related events (SREs) has been evaluated in multiple randomized clinical trials for patients with nonmetastatic castration-sensitive prostate cancer (CSPC). One study demonstrated a significant decrease in BMD in men receiving ADT alone, while there was no significant change in those who received ADT plus pamidronate.[16] In castration-resistant prostate cancer (CRPC) metastatic to bone, a randomized placebo-controlled trial found that zoledronic acid reduced SREs.[17] Another phase III randomized clinical trial found denosumab to be more effective than zoledronic acid in preventing SREs.[18] Interestingly, in contrast to men with metastatic CRPC, no benefit was seen from osteoclast inhibition in men with CSPC metastatic to bone.[19]
Men who are about to start ADT should be evaluated for risk of osteoporosis, prior fractures, alcohol use, and prior (or current) glucocorticoid use. Serum vitamin D and baseline BMD may be checked to see if bisphosphonates are indicated, with periodic re-evaluation of BMD while on ADT. For all patients starting ADT, it is recommended that they supplement their diet with at least 1,000-mg oral calcium daily and 1,000 IU of vitamin D in an effort to preserve bone integrity and minimize losses; a referral to a registered dietician may further aid in refining both dietary and supplement recommendations. Lastly, an exercise program that includes resistance training and/or weight-bearing exercise is encouraged to further maintain bone strength.
Metabolic Syndrome
A variety of metabolic changes have been observed with ADT, including weight gain, dyslipidemia, hyperglycemia, and sarcopenia. Weight gain, specifically, is a well-recognized side effect of ADT.[20-22] Retrospective studies have found that men on ADT for nonmetastatic prostate cancer had a median weight gain of 1 to 2 kg after 1 year of treatment.[22] Similar changes in weight have been noted in the metastatic setting.[23-25] When more dramatic, weight gain can have major consequences in terms of both mental and cardiovascular health. A referral to a registered dietician may help with improving diet, while engagement in a structured and formal exercise program can help with reducing or maintaining weight. Many cancer centers offer such programs, and these should be suggested to interested or at-risk patients.
In addition, multiple studies have noted dyslipidemia and increased risk for metabolic syndrome with use of ADT.[26,27] Extrapolating that these changes are associated with increases in cardiovascular risk remains controversial. Loss of lean muscle mass and sarcopenic obesity have been described in several studies. A study of 39 men receiving ADT using CT measurements of the rectus, femoris, sartorius, and quadriceps muscles noted decreases in the cross-sectional area of these muscles.[28] Given the importance of these muscles in gait and balance, studies have explored the association between ADT use and fall risk. One study noted a higher rate of falls in persons treated with ADT, with apparent persistent risk even after ADT is discontinued.[29] Thus, judicious use of ADT and careful evaluation of frail patients and those at risk for complications are recommended when the need for treatment is questionable (eg, biochemical relapse with slowly rising prostate-specific antigen [PSA] levels).
Neurocognitive Changes
Emerging data show that men with prostate cancer receiving ADT are at risk for a spectrum of neurocognitive complications, such as depression, memory difficulties, and fatigue.[30] In a population-based cross-sectional study of elderly men, it was found that lower serum testosterone levels were associated with decreased performance on the Mini-Mental State Examination (MMSE), the Trail Making Test B, and the Digit Symbol Substitution cognitive test. A major confounding variable in this study was age, since more than half of all cases of dementia occur in men > 65 years of age. This was addressed in a large cohort study that found a statistically significant association between use of ADT and risk of dementia.[31] Sensitivity analyses found that use of ADT for longer than 12 months was associated with the greatest absolute risk of dementia.
Numerous prospective studies examining the impact of ADT on cognitive function have been performed, with mixed and conflicting results. A prospective study of men with extraprostatic disease randomized 82 patients to receive either leuprolide, goserelin, cyproterone acetate, or close clinical monitoring. All patients underwent serial cognitive assessments at baseline, at the start of treatment, and at 6 months.[32] A decrease in cognitive performance after 6 months of ADT use was found in the patients on active treatment compared with those on the close monitoring arm. A major limitation of this study is that spatial memory testing was omitted from the analysis, which has been shown to be more sensitive in detecting cognitive differences.[33] Another cross-sectional study compared neuropsychological parameters in three groups of patients: patients with prostate cancer receiving ADT, patients with prostate cancer not receiving ADT, and normal controls.[34] Here, the authors made a distinction between time-based prospective memory (eg, remembering to call a friend in 1 hour) and event-based prospective memory (eg, remembering to buy fruit when passing a fruit stand). This study demonstrated that men receiving ADT did demonstrably worse in event-related prospective memory than men not receiving ADT and matched controls. A limitation of this study was the lack of long-term follow-up on cognitive function, making it difficult to know whether the neurocognitive effects of ADT persist after discontinuation of therapy.
These studies can be contrasted with several others that have not demonstrated an association between use of ADT and neurocognitive decline. A large cohort study compared cognitive function using neuropsychological tests in the following groups: men with prostate cancer receiving continuous ADT, men with prostate cancer not receiving ADT, and healthy controls.[35] The authors found no difference in cognitive function over 12 months of ADT use. Furthermore, a recent large meta-analysis failed to find an association between cognitive impairment and ADT.[36] Similar findings were reported in one of the largest population studies of this kind, which examined 1.2 million Medicare beneficiaries who developed prostate cancer from 2001 to 2014.[37] The risk of dementia was not associated with duration of ADT (ie, there was no dose-dependent effect). Currently, there is mixed evidence on whether ADT is associated with long-term neurocognitive impairments, and this remains a topic of active research. In patients with baseline cognitive impairment, it is reasonable to attempt to minimize exposure to ADT, if possible (through intermittent treatment or by treating with anti-androgen monotherapy).
Thrombotic Complications
Thromboembolic risk has been noted in several studies.[31,38] In a large retrospective series, patients who received ADT had a 15% absolute risk of venous thromboembolism (VTE), compared with 7% among patients who did not receive ADT. Overall, there was a significant association between ADT use and risk of VTE or arterial embolism (adjusted hazard ratio [HR], 1.56; 95% CI, 1.50–1.61; P < .0001). Furthermore, greater duration of ADT was associated with an increased number of VTE events. These data are especially important to consider in patients with additional risk factors for VTE. Indeed, as indicated previously, tamoxifen has been reported to be useful therapy for ADT-associated gynecomastia,[13] yet it is an independent risk factor for thrombosis. Breast irradiation can be an alternative in symptomatic patients with thrombotic risk.
Data regarding use of ADT and risk of stroke are conflicting. A prospective case-control study from Taiwan reported no increased risk of stroke in patients with prostate cancer receiving ADT vs those not receiving it in an adjusted analysis.[39] In contrast, a meta-analysis reported a trend toward increased risk of stroke with ADT; however, this was not statistically significant (HR, 1.12; 95% CI, 0.95–1.32; P = .16). That said, subgroup analysis did identify GnRH agonist use alone or combined with anti-androgen use, and surgical castration, as having a significant association with stroke.[40] Based on the available evidence, risk of stroke should be mentioned when obtaining informed consent; however, the individual absolute risk is likely low.
Cardiovascular Complications
There are conflicting data on the risk of cardiovascular disease (CVD) with use of ADT. Currently, there are no prospective randomized controlled data assessing the association of ADT use with risk of CVD. In a large retrospective population-based cohort study, multivariate analyses demonstrated that men with newly diagnosed prostate cancer who received ADT had a 20% increased risk of CVD.[41] Somewhat paradoxically, the study found that men receiving treatment for less than 12 months were at higher risk for cardiovascular events compared with men who had been on ADT for longer. A major limitation of this study is that the researchers were unable to control for smoking and obesity, which are two major risk factors for CVD and could confound the results. Additionally, age was a major variable associated with CVD. A meta-analysis of eight large trials found no significant differences in risk of CVD in patients receiving ADT vs controls, nor was duration of ADT significantly associated with increased risk of CVD.[42]
KEY POINTS
- Vasomotor complications are common in men receiving androgen deprivation therapy (ADT) and can be mitigated by pharmacologic and nonpharmacologic strategies.
- There is an increased risk of osteoporosis and skeletal-related events in men receiving ADT. Calcium and vitamin D supplements should be offered to all patients. Osteoclast inhibitors should be considered in men at high risk for osteoporotic fractures and men with metastatic castration-resistant prostate cancer.
- Evidence on the association between ADT use and neurocognitive decline and cardiovascular disease remains mixed and controversial.
- Multidisciplinary management with specialists and allied health professionals may assist in managing the complex side effects of ADT.
Currently, no specific recommendation adjustments for men with prostate cancer receiving ADT should be pursued outside of primary prevention, including smoking cessation, and secondary prevention, including glycemic control, lipid-lowering therapy, and aspirin therapy for men with coronary artery disease. Given the propensity of patients on ADT to gain central adiposity, a healthy diet and exercise program are recommended to all patients at the start of treatment. Intermittent ADT or antiandrogen monotherapy may be appropriate for select patients (eg, those with biochemical relapse, low burden of metastases with more indolent course, and deep PSA nadir) at high risk for cardiovascular events; such patients should be evaluated on an individual basis and engaged in shared decision making, weighing the risk of a cardiovascular event vs cancer progression. Ultimately, patients with known CVD or those with numerous CVD risk factors should be evaluated promptly, if they develop new symptoms of chest pain or dyspnea while on ADT. A referral to cardio-oncology may assist in risk stratification.
Renal Complications
Observational data suggest an association between ADT use and rate of acute kidney injury (AKI).[43,44] In retrospective studies, the link appeared stronger with use of GnRH agonists plus an antiandrogen, as well as with GnRH agonists alone, compared with surgical castration; however, the inherent biases within such studies and the potential for numerous confounders raise questions regarding causality and the strength of association. Thus, use of ADT may present an increased risk of AKI, although the true risk and clinical significance are difficult to quantify.
Conclusion
ADT is the cornerstone of management for men with metastatic prostate cancer. It is associated with numerous side effects that can influence quality of life. Hot flushes, sexual dysfunction, gynecomastia, osteoporosis, metabolic syndrome, and depression are well-described complications of ADT. The implications of ADT use for risks of neurocognitive decline and CVD remain controversial, with multiple studies documenting conflicting results. Addressing quality-of-life concerns is of paramount importance with use of ADT, given the increased survival benefits found with combinations of ADT with other agents. Given the advanced age of many patients and the prolonged duration of ADT when treating localized disease with curative intent, some patients remain hypogonadal long after completion of therapy, underscoring the potential long-lasting sequelae of treatment. While consensus is lacking, there are mounting data[45] suggesting that testosterone replacement therapy may be cautiously used in select individuals in whom risk of prostate cancer relapse is determined to be low and hypogonadism remains long after ADT cessation. Ultimately, applying a multidisciplinary care model that incorporates specialists and allied healthcare professionals to aid in pharmacologic and lifestyle interventions is likely to provide optimal benefit in managing side effects for patients receiving long-term ADT.
Financial Disclosure:The authors have no significant financial interest in or other relationship with the manufacturer of any product or provider of any service mentioned in this article.
References:
1. Sartor O, de Bono JS. Metastatic prostate cancer. N Engl J Med. 2018;378:645-57.
2. Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294:238-44.
3. Holzbeierlein JM, McLaughlin MD, Thrasher JB. Complications of androgen deprivation therapy for prostate cancer. Curr Opin Urol. 2004;14:177-83.
4. Smith JA Jr. Management of hot flushes due to endocrine therapy for prostate carcinoma. Oncology (Williston Park). 1996;10:1319-22; discussion 24.
5. Irani J, Salomon L, Oba R, et al. Efficacy of venlafaxine, medroxyprogesterone acetate, and cyproterone acetate for the treatment of vasomotor hot flushes in men taking gonadotropin-releasing hormone analogues for prostate cancer: a double-blind, randomised trial. Lancet Oncol. 2010;11:147-54.
6. Loprinzi CL, Dueck AC, Khoyratty BS, et al. A phase III randomized, double-blind, placebo-controlled trial of gabapentin in the management of hot flashes in men (N00CB). Ann Oncol. 2009;20:542-9.
7. Shanafelt TD, Barton DL, Adjei AA, Loprinzi CL. Pathophysiology and treatment of hot flashes. Mayo Clin Proc. 2002;77:1207-18.
8. Beer TM, Benavides M, Emmons SL, et al. Acupuncture for hot flashes in patients with prostate cancer. Urology. 2010;76:1182-8.
9. Alemozaffar M, Regan MM, Cooperberg MR, et al. Prediction of erectile function following treatment for prostate cancer. JAMA. 2011;306:1205-14.
10. Ferrer M, Suarez JF, Guedea F, et al. Health-related quality of life 2 years after treatment with radical prostatectomy, prostate brachytherapy, or external beam radiotherapy in patients with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;72:421-32.
11. Gay HA, Sanda MG, Liu J, et al. External beam radiation therapy or brachytherapy with or without short-course neoadjuvant androgen deprivation therapy: results of a multicenter, prospective study of quality of life. Int J Radiat Oncol Biol Phys. 2017;98:304-17.
12. Tunio MA, Al-Asiri M, Al-Amro A, et al. Optimal prophylactic and definitive therapy for bicalutamide-induced gynecomastia: results of a meta-analysis. Curr Oncol. 2012;19:e280-e288.
13. Viani GA, Bernardes da Silva LG, Stefano EJ. Prevention of gynecomastia and breast pain caused by androgen deprivation therapy in prostate cancer: tamoxifen or radiotherapy? Int J Radiat Oncol Biol Phys. 2012;83:e519-e524.
14. Higano CS. Bone loss and the evolving role of bisphosphonate therapy in prostate cancer. Urol Oncol. 2003;21:392-8.
15. Shahinian VB, Kuo YF, Freeman JL, Goodwin JS. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med. 2005;352:154-64.
16. Smith MR, McGovern FJ, Zietman AL, et al. Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer. N Engl J Med. 2001;345:948-55.
17. Saad F, Gleason DM, Murray R, et al. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94:1458-68.
18. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet Oncol. 2011;377:813-22.
19. Smith MR, Halabi S, Ryan CJ, et al. Randomized controlled trial of early zoledronic acid in men with castration-sensitive prostate cancer and bone metastases: results of CALGB 90202 (Alliance). J Clin Oncol. 2014;32:1143-50.
20. Braunstein LZ, Chen MH, Loffredo M, et al. Obesity and the odds of weight gain following androgen deprivation therapy for prostate cancer. Prostate Cancer. 2014;2014:230812.
21. Kim HS, Moreira DM, Smith MR, et al. A natural history of weight change in men with prostate cancer on androgen-deprivation therapy (ADT): results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. BJU Int. 2011;107:924-8.
22. Seible DM, Gu X, Hyatt AS, et al. Weight gain on androgen deprivation therapy: which patients are at highest risk? Urology. 2014;83:1316-21.
23. Mitsuzuka K, Kyan A, Sato T, et al. Influence of 1 year of androgen deprivation therapy on lipid and glucose metabolism and fat accumulation in Japanese patients with prostate cancer. Prostate Cancer Prostatic Dis. 2016;19:57-62.
24. Salvador C, Planas J, Agreda F, et al. Analysis of the lipid profile and atherogenic risk during androgen deprivation therapy in prostate cancer patients. Urol Int. 2013;90:41-4.
25. Torimoto K, Samma S, Kagebayashi Y, et al. The effects of androgen deprivation therapy on lipid metabolism and body composition in Japanese patients with prostate cancer. Jpn J Clin Oncol. 2011;41:577-81.
26. Bosco C, Crawley D, Adolfsson J, et al. Quantifying the evidence for the risk of metabolic syndrome and its components following androgen deprivation therapy for prostate cancer: a meta-analysis. PLoS One. 2015;10:e0117344.
27. Braga-Basaria M, Dobs AS, Muller DC, et al. Metabolic syndrome in men with prostate cancer undergoing long-term androgen-deprivation therapy. J Clin Oncol. 2006;24:3979-83.
28. Chang D, Joseph DJ, Ebert MA, et al. Effect of androgen deprivation therapy on muscle attenuation in men with prostate cancer. J Med Imaging Radiat Oncol. 2014;58:223-8.
29. Winters-Stone KM, Moe E, Graff JN, et al. Falls and frailty in prostate cancer survivors: current, past, and never users of androgen deprivation therapy. J Am Geriatr Soc. 2017;65:1414-9.
30. Shahinian VB, Kuo YF, Freeman JL, Goodwin JS. Risk of the ‘androgen deprivation syndrome’ in men receiving androgen deprivation for prostate cancer. Arch Intern Med. 2006;166:465-71.
31. Nead KT, Gaskin G, Chester C, et al. Association between androgen deprivation therapy and risk of dementia. JAMA Oncol. 2017;3:49-55.
32. Green HJ, Pakenham KI, Headley BC, et al. Altered cognitive function in men treated for prostate cancer with luteinizing hormone-releasing hormone analogues and cyproterone acetate: a randomized controlled trial. BJU Int. 2002;90:427-32.
33. Cherrier MM, Asthana S, Plymate S, et al. Testosterone supplementation improves spatial and verbal memory in healthy older men. Neurology. 2001;57:80-8.
34. Yang J, Zhong F, Qiu J, et al. Dissociation of event-based prospective memory and time-based prospective memory in patients with prostate cancer receiving androgen-deprivation therapy: a neuropsychological study. Eur J Cancer Care (Engl). 2015;24:198-204.
35. Alibhai SM, Breunis H, Timilshina N, et al. Impact of androgen-deprivation therapy on cognitive function in men with nonmetastatic prostate cancer. J Clin Oncol. 2010;28:5030-7.
36. Sun M, Cole AP, Hanna N, et al. Cognitive impairment in men with prostate cancer treated with androgen deprivation therapy: a systematic review and meta-analysis. J Urol. 2018;199:1417-25.
37. Baik SH, Kury FSP, McDonald CJ. Risk of Alzheimer’s disease among senior Medicare beneficiaries treated with androgen deprivation therapy for prostate cancer. J Clin Oncol. 2017;35:3401-9.
38. Ehdaie B, Atoria CL, Gupta A, et al. Androgen deprivation and thromboembolic events in men with prostate cancer. Cancer. 2012;118:3397-406.
39. Chung SD, Chen YK, Wu FJ, Lin HC. Hormone therapy for prostate cancer and the risk of stroke: a 5-year follow-up study. BJU Int. 2012;109:1001-5.
40. Meng F, Zhu S, Zhao J, et al. Stroke related to androgen deprivation therapy for prostate cancer: a meta-analysis and systematic review. BMC Cancer. 2016;16:180.
41. Saigal CS, Gore JL, Krupski TL, et al. Androgen deprivation therapy increases cardiovascular morbidity in men with prostate cancer. Cancer. 2007;110:1493-500.
42. Nguyen PL, Alibhai SM, Basaria S, et al. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur Urol. 2015;67:825-36.
43. Gandaglia G, Sun M, Hu JC, et al. Gonadotropin-releasing hormone agonists and acute kidney injury in patients with prostate cancer. Eur Urol. 2014;66:1125-32.
44. Lapi F, Azoulay L, Niazi MT, et al. Androgen deprivation therapy and risk of acute kidney injury in patients with prostate cancer. JAMA. 2013;310:289-96.
45. Golla V, Kaplan AL. Testosterone therapy on active surveillance and following definitive treatment for prostate cancer. Curr Urol Rep. 2017;18:49.