Doxorubicin-Eluting Beads Used for Chemoembolization
When patients with hepatocellular carcinoma (HCC) still have viable tumor after radiofrequency ablation (RFA), further treatment with chemoembolization using doxorubicin-eluting beads increases the ablation volume by an average of 61%,
SEATTLEWhen patients with hepatocellular carcinoma (HCC) still have viable tumor after radiofrequency ablation (RFA), further treatment with chemoembolization using doxorubicin-eluting beads increases the ablation volume by an average of 61%, new data show. Moreover, the combined treatment is associated with an objective complete response rate of 70%.
Riccardo Lencioni, MD, of the Diagnostic and Interventional Radiology Oncology Department, University of Pisa, presented the data at the 32nd Annual Meeting of the Society of Interventional Radiology (abstract 125).
Study Rationale
Describing the rationale for the study, Dr. Lencioni said that its design was based on selective delivery of drug-eluting beads only to viable tumor, exploitation of the hyperemia induced by RFA (which both enhances peritumoral blood flow and facilitates angiographic intravascular targeting), and capitalization on the damage induced to any residual viable tumor by sublethal heating. These factors collectively produce higher drug concentrations in the tumor, sustained drug release and activity, and greater susceptibility of the tumor cells to the chemotherapeutic agent, Dr. Lencioni said.


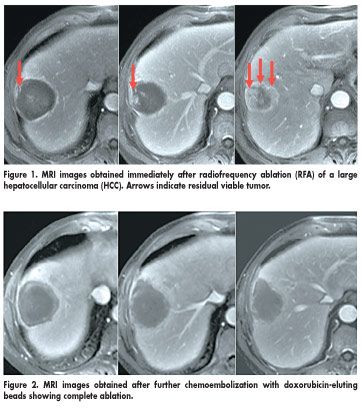
Study participants were 20 patients who had uninodular HCCs larger than 3 cm in diameter and unequivocal evidence of residual viable tumor on CT or MRI scans obtained immediately after RFA. Within 24 hours, the patients underwent Precision TACE (transarterial chemoembolization) with drug-eluting beads (DC Bead, Biocompatibles International, Farnham, UK) loaded with doxorubicin. (DC Beads are investigational in the United States.)
"We aimed at delivering selectively the DC Beads to the viable portion of the tumor, assuming that most of the tumor had already been ablated due to the use of RFA, and at possibly being able to increase the effect particularly at the periphery and particularly at any possible microsatellite or microangioinvasion," Dr. Lencioni said. Scans were obtained again at 1 month and then every 3 months thereafter. The mean diameter of tumors before treatment was 5 cm (range, 3.3 to 7 cm). "The treatment was quite safe," Dr. Lencioni commented. "We had no major complications, no severe adverse events in the study." Mean follow-up was 9.0 ± 4.5 months.
Increased Ablation Volume
Compared with the mean ablation (coagulative necrosis) volume obtained immediately after RFA, that obtained after further treatment with doxorubicin-eluting beads was greater by a relative 61%, he said.
According to EASL (European Association for the Study of the Liver) criteria, 14 of 20 patients (70%) had an objective complete response, and 6 patients (30%) had an objective partial response with the combined treatment.
Dr. Lencioni further noted that combined treatment was not only beneficial for larger tumors but also for those in difficult locations. Overall estimated 1-year survival is 100%.
"To sum up our data, with this preliminary analysis, we have a proof of a concept: It is possible to substantially increase the volume of ablation when the tumor area is exposed to such high concentrations of doxorubicin as provided by the use of doxorubicin-eluting beads," Dr. Lencioni concluded.
He added that although early response and survival results are promising with the therapy, longer follow-up will be needed.















