Mayo Clinic on AE Management Strategies for EGFR-Mutated NSCLC
The combination of amivantamab plus lazertinib has emerged as a potential treatment option for patients with EGFR-mutated NSCLC and has shown sufficient efficacy responses.


The combination of amivantamab plus Lazertinib has emerged as a potential treatment option for patients with EGFR-mutated NSCLC and has shown sufficient efficacy responses.
Experts from the Mayo Clinic in Rochester, MN, discussed how the addition of the phase 3 MARIPOSA [NCT04487080] regimen of amivantamab-rmjw (Rybrevant) plus lazertinib (Lazcluze) has emerged as a treatment option compared with osimertinib (Tagrisso).1
The panel was led by Konstantinos Leventakos, MD, PhD, a medical oncologist with a focus in thoracic malignancies. Additional members included Harry Fuentes, MD, consultant and assistant professor; Kadi Studeck, MD, a medical oncologist; Kaushal Parikh, MD, a medical oncologist involved in early therapeutics; Ailsa Luce, PA-C, a physician assistant; Tammy O'Brien, NP, a nurse practitioner; Tassos Dimou, MD, a medical oncologist; and Mohammed Shanshal, MB, BCh, MD, a medical oncologist.
Additionally, the panel also discussed recent clinical trials involving amivantamab given either intravenously (IV) or subcutaneously plus lazertinib which have demonstrated valuable insights into these immune-related adverse effects (AEs). Moving forward, the experts discussed how to adapt their strategies to involve the prevention of these AEs.
Amivantamab Plus Lazertinib Combination
Leventakos: The early clinical trial activity of amivantamab and lazertinib was with all 20 patients on the trial responding to amivantamab and lazertinib, and that was the phase 1 CHRYSALIS [NCT02609776] trial.2 There were 20 patients with treatment naïve EGFR, [and EGFR exon19 deletion/L858R]. At almost 3 years, 10 out of 20 patients were still receiving ongoing treatment. This trial led to the MARIPOSA study design. This is one of the most famous studies of the last year, and it also got FDA approval in August [2024].3
For this study, we have locally advanced metastatic, exon 19 or L858R, stratified based on mutation, history of brain metastasis, or not. There are 3 arms that were randomly assigned 2:2:1 to amivantamab and lazertinib or osimertinib. The lazertinib arm was included mainly because the FDA wanted to have the contributor of the primary end point of progression- free survival [PFS]. This would be the amivantamab and lazertinib vs osimertinib, with secondary end points of overall survival, response rate, duration of response, PFS after PFS2, symptomatic PFS, intracranial PFS, and safety.
For PFS an HR of 0.70 [95% CI, 0.58-0.85; P <.001] was observed. At 2 years, the PFS rates were 48% in the amivantamab and lazertinib arm compared with 34% in the osimertinib arm. For the overall response rate, 86% [95% CI, 83%-89%] vs 85% [95% CI, 81%-88%], and confirmed responders of 80% [95% CI, 76%-84%] and 76% [95% CI, 71%-80%]. There were ongoing responses of 62% vs 48%. When it comes to the patients who are responding, we see more patients responding with amivantamab and lazertinib, for at least up to 27 to 30 months. When we look into the longer-term follow-up and intracranial PFS, up to 24 months, the difference is about 51% vs 48%. At 36 months, in this third year, there is a big differentiation that looks into the 38% vs 18%.
When it comes to the first subsequent therapy, if we look at what patients got after they progressed, of course, fewer patients progressed on amivantamab and lazertinib. We can see that doublet chemotherapy was what was chosen by the majority of patients. Doublet chemotherapy and immunotherapy or VEGF were coming second for the osimertinib arm. The PFS after the first subsequent therapy, based on what the patient had before, we see that amivantamab and lazertinib had a statistically significant HR of 0.73 [95% CI, 0.59-0.91; P = .004]. Even with the second treatment, these patients might still have a better PFS. When it comes to the overall survival of MARIPOSA to the point that we have data up to now, it seems that the difference at 3 years was 61% vs 53% for these patients.
When it comes to key adverse effects [AEs] over time, when we look into patients who had interruptions or who didn’t have interruptions, we can all agree that the first 4 months are a little more busy than the second 4 months. The most common AEs were classic EGFR things like rash and paronychia. We have stomatitis, decreased appetite, some edema, and diarrhea.
What about the patients who had dose interruptions? For the patients who have any dose interruptions, if I need to decrease the dose or interrupt the dose, does it have some impact? It seems that there was not a significant impact on how the patients did. Now that we have a little more general idea of MARIPOSA efficacy and safety, what happens when patients progress, what are your thoughts on this updated data, maybe with a little of the trend of overall survival?
Dimou: The efficacy data look very similar to the phase 3 FLAURA2 [NCT04035486], but certainly the toxicity is different, not necessarily better or worse, but different.4 We get more cytopenias with the FLAURA2 and more EGFR and MET-related toxicity with the MARIPOSA regimen. In my experience, the use of amivantamab is difficult when we use it in the second line as part of the phase 3 MARIPOSA-2 [NCT04988295] regimen with chemotherapy and amivantamab.5 It’s also heavy in terms of the required supportive care, which is important for those patients who have to address those AEs with a whole bag of drugs. It’s not like we’re giving them 1 or 2 antineoplastics. We’re giving them supportive treatment, which can be overwhelming. I don’t have a lot of experience with the amivantamab plus lazertinib regimen yet, but in general, the chemotherapy plus osimertinib [regimen] would be easier, has less visits to the office or to the infusion center, and less supportive care that is required. The effectiveness appears to be the same. I don’t see the reason why we would prioritize the MARIPOSA regimen. I don’t know what my colleagues think.


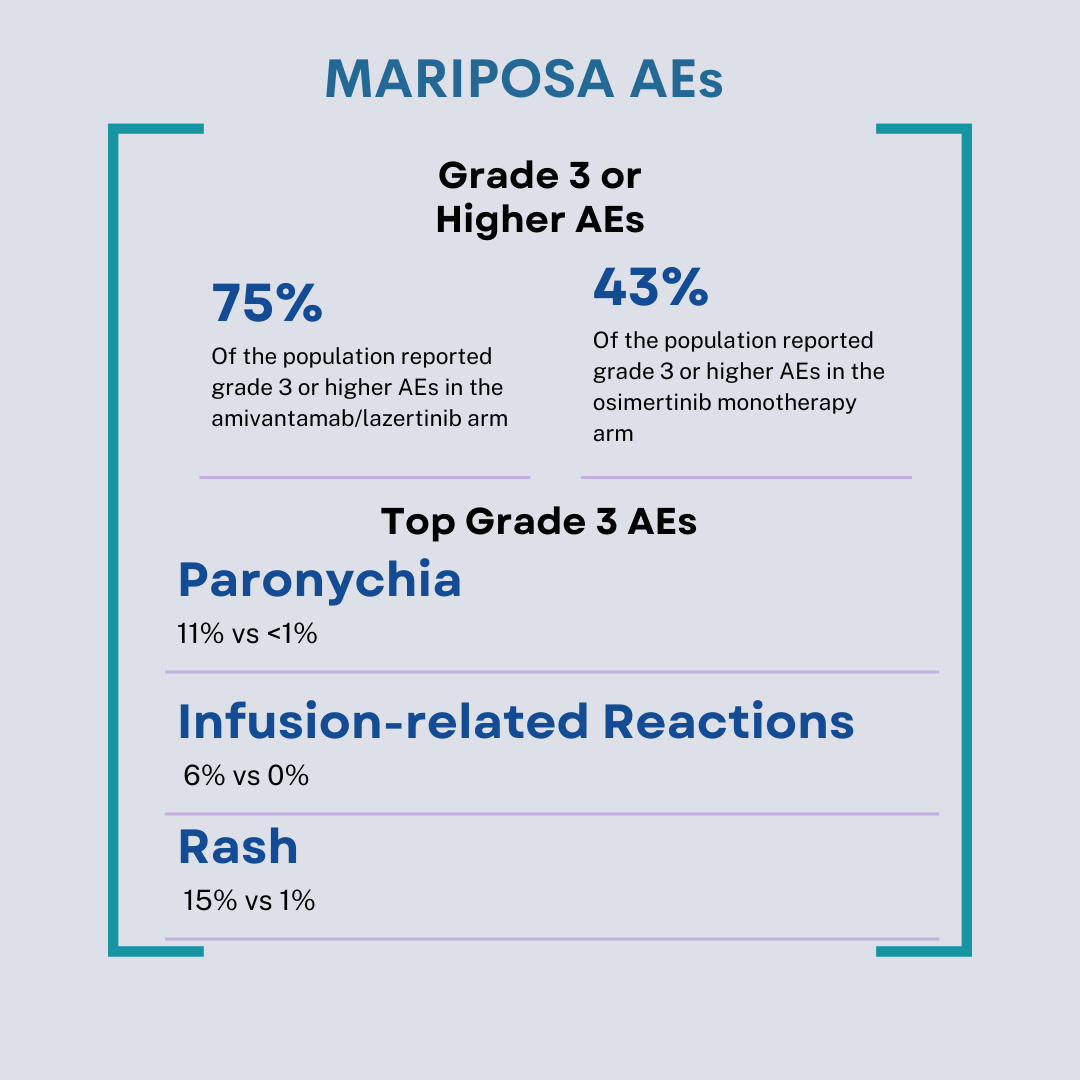
The most prevalent AEs from the MARIPOSA trial.
Parikh: First of all, the data are impressive. Patients with positive ctDNA had an arbitrary cut-off, maybe 1% or greater VAF had a greater benefit with chemotherapy plus osimertinib vs osimertinib monotherapy. That’s something you see here as well: patients who have positive ctDNA clearance. It’s hard to predict, as you mentioned earlier. I find it challenging to fit this regimen [of amivantamab plus lazertinib] in my first-line practice right now for a couple of reasons. Certainly, tolerability is key. The amount of time that patients need to be in [to receive the treatment] early on in the course of their diagnosis. Financial toxicity, as it's much more expensive than carboplatin plus pemetrexed. The other thing with carboplatin plus pemetrexed is that it’s 4 cycles of treatment. You look at pemetrexed, on average, patients with a median number of cycles were 8 to 9 cycles. The toxicity associated with single-agent maintenance pemetrexed is something we are well used to. We are well-versed in how to manage cytopenias, whether it’s by dose reduction dose delay, growth factor support, or even withholding [treatment].
Would subcutaneous amivantamab drastically change this paradigm? It will improve the [amount of time in the] chair from the infusion reaction perspective. Infusion reaction is something we’ve got a good handle on how to manage those. I’m not sure how that changes the rash and the paronychia and those AEs because the phase 3 PALOMA 3 [NCT05388669] trial had very similar rates of those AEs.6 Right now, it’s challenging to fit this regimen over FLAURA2. We’ll see what overall survival and the curves are separating very nicely. In my experience, patients, while they don’t want a drug to be intolerable, they value overall survival more than tolerance. Especially these patients who are generally otherwise healthier, younger, fitter, and often have young families.
Leventakos: What is your general approach to frontline treatment? What factors do you consider when making the treatment decisions?
Shenshel: There are multiple factors there. One of them is the functional status of the patient, medical eligibility, and whether they’re physically fit to go for any of those treatments. We have many good options between osimertinib, osimertinib plus chemotherapy, and amivantamab plus lazertinib. [First], is the patient eligible? What are the co-mutations to consider, as well as the volume of the disease? The last thing I put in mind is that this is all based on the biopsy itself and is not representative of the whole.
You have an adenocarcinoma, you have a clone of EGFR, but you could have other histology going on there. Because of that, in any medically fit patient, my preference is to consider chemotherapy plus osimertinib, which could explain why those patients perform better. If we look at the HR, although we don’t want to do a cross-trial comparison between those 2, the HR is 0.65, and the chemotherapy plus osimertinib is even a little bit better than the amivantamab plus lazertinib. That’s what I think in the back of my head. I discussed with the patient as much, explaining between these 2 options, what is the rationale, what the risk is, and what’s the benefits. Otherwise, in patients who are older, and not medically fit, osimertinib is the way to go to avoid any of those systemic toxicity. The last thing is whether the patient can logistically commit to extra treatment, extra infusions, whether it’s chemotherapy or amivantamab vs the convenience of osimertinib?
Parikh: When we talk about financial toxicity, we also have to mention that these patients who start amivantamab need 4 months of anticoagulation. Often, we are using newer direct oral anticoagulants. These are some of the most expensive drugs that we have on the market. Often, we’ve had patients who are not approved for rivaroxaban [Xarelto] or apixaban [Eliquis] and had a co-pay of $3,000 a month.
Shenshel: I’m glad you mentioned that. We did an analysis of the financial costs of osimertinib, and found it’s a substantial difference vs amivantamab.
Prophylactic Measures and AE Management
Leventakos: The phase 2 SKIPPirr study [NCT05663866] looked into 4 different independent prophylactic strategies for patients who were receiving amivantamab and or lazertinib.7 The prophylactic here had to do mainly with the reactions that this patient had. One was dexamethasone at 4 mg, dexamethasone at 8 mg, montelukast at 10 mg, and methotrexate at 25 mg. They looked into [using] Simon’s 2-stage [design], and if there was an infusion reaction in 3 patients or less, then they could [enroll more patients].
The 4 mg of dexamethasone and 25 mg of methotrexate did not pass stage 1 [of enrolling 6 patients]. The montelukast did not make it to stage 2 [of enrolling 10 patients]. The prophylaxis of dexamethasone 8 mg passed both stages, went to the expansion stage, and enrolled 24 additional patients. With dexamethasone prophylaxis, they were able to reduce the amivantamab [immune-related reaction (IRR) rate] by 22.5%. The prophylactic schedule is [to take] 2 days [before] and 1 day before for dexamethasone at 8 mg in the morning and in the afternoon, and then in the clinic, you get the amivantamab, and you see how [the IRR rate] went from 67.4% to 22.5%.
At the Mayo Clinic, we are blessed to have the most amazing pharmacists, who have taken all this burden of [dosing], which is huge for the care of the patients, but it's interesting to see how some things can change everything, and you see how dexamethasone decreased a lot of AEs. As a reminder, dexamethasone and the other steroids were found at Mayo Clinic, in case we don't remember that. What are some of the strategies that you have in place to manage IRR? Do we have prophylactic supportive measures in place? How would you implement this 8 mg dexamethasone?
Parikh: We don’t need subcutaneous amivantamab anymore?
Leventakos: It is OK that we have maximized everything that would make it easier for the patient. At least the practice at Mayo Clinic is fully updated. We have been giving amivantamab for a long time. We had the first clinical trial here. We have nailed it so far. Would the SKIPPirr trial bringing the reactions from 67.4% to 22.5% make anybody more comfortable incorporating the amivantamab earlier in our practice? Talking to a practice, who has probably nailed everything that has to do with the infusion reaction so far.
Dimou: There is still a lot of toxicity with amivantamab, and supportive care needs to be given. It’s not just the toxicity; it’s also the supportive care that can overwhelm patients. The antibiotics, creams, and shampoos are a lot. Although it is certainly better with a modified pretreatment in terms of the infusion reaction; that’s one thing--there are many others. I wouldn’t change my approach towards amivantamab to prefer it for the later line, or second line.
Leventakos: The PALOMA-3 trial was an open-label, randomized study that looked into subcutaneous amivantamab and lazertinib compared with IV amivantamab.The subcutaneous amivantamab was given 1600 mg weekly for 4 weeks, then every 2 weeks. The comparator arm has matched dosing but was given through an IV. Prophylactic anticoagulation was recommended in both studies. [The results were] mainly pharmacokinetic but had secondary end points of response rate for low inferiority progression-free survival [PFS] and overall survival [OS].
We see that the pharmacokinetics were good. When it comes to efficacy, we have the results that showed that the subcutaneous duration of response was higher than with the IV. PFS was higher, with a good HR. Everybody was a little surprised by that because they went from low inferiority to something that showed that things were even better. When it comes to the safety issues with IRRs, it went down from 66% to 13%, with a huge increase in grade 3 or higher [AEs]. At the median follow-up of 7 months, [the trial] had met both co-primary end points of pharmacokinetics.
There is another phase 2 trial, the COCOON trial [NCT06120140], that looked into dermatologic management with first-line [amivantamab plus lazertinib].8 That speaks to what Dr Dimou said: that it's not only the IRRs, but all the dermatologic [AEs]. We will be working on that. One practical consideration of amivantamab is that we always remember the most common AEs. There are the IRRs in everything that has to do with EGFR. There are warnings and precautions for IRRs, interstitial disease or pneumonitis, dermatologic AEs, ocular toxicity, and [embryonal-fetal toxicity]. How does the team think that the proactive strategies for managing toxicities are for amivantamab?
Shanshal: I can commend that. It’s very important to maximize it more, especially with the PFS and OS benefits in this case. If you look at the way that it’s given, you start with a low dose and then you [increase] the dosing. Minimizing the allergic AEs of it and minimizing the immediate toxicity is paramount for importance so that you can proceed with the subsequent escalation of the dosing in this case. Also, compliance with the rate of discontinuation will decrease with the management of those AEs, which the majority of them are more for the engager part that’s inducing it, including the rash and perineum care, et cetera. Compliance from the patients can transmit an improvement in the PFS and OS of the patient.
Leventakos: Any practical tips for implementing these proactive strategies into the clinical practice?
Dimou: Get a thoracic pharmacist.
Leventakos: That brings up the next thing, which was what are the challenges that might arise with integrating proactive management strategies, and what tools and resources [might you use]? You both mentioned that we are blessed to have a thoracic oncology pharmacist, who has been doing the COCOON and the SKIPPirr [regimens] before they were even accepted.
It comes to something else that nobody openly talks about, which is time toxicity, not only for the patient but also for the care team because it's different. Our resources are limited, and having to deal with AEs for 3 hours is a different burden than having to deal with AEs for 10 minutes. Changing the education of the whole care team is something new because our brains have been studying for so many years, and we know how to get things, but still, it takes time. It doesn’t only have to work, but it also has to be easy. This amount of easiness is something that we try to capture in different ways in quality of life. We are blessed to have an amazing supportive team for us when using amivantamab. I don’t remember the last time that I had to deal with an IRR.
How much did this data change your opinion about the first-line [amivantamab]? The main data that I would like to bring up is that reactions are manageable; probably for dermatologic toxicity, there will be something better, and for subcutaneous, something is coming. How do you feel about changing your first-line or your second-line [therapy] right now? What would make you change your second-line?
Shanshal: The main question is, what would be the sequence here? To me, I still prefer the chemotherapy plus osimertinib [Tagrisso]. Having said that, the data for subcutaneous amivantamab is promising. If you look at the OS benefit and the HR, and that goes down to the mechanism function of this drug, there is also some natural killer activation. I’m wondering if this has to do with the lymphatic uptake. I’m looking closely at the subcutaneous data as a very convenient option for those patients as well. Until then, I still prefer chemotherapy plus osimertinib.
Parikh: It makes sense to prefer subcutaneous over IV. One question to ask is, would you still consider single-agent osimertinib in any of these patients in the frontline? There are prospective trials ongoing. I’d be very curious to see if those patients who have positive ctDNA at the third cycle and get 2 or 4 cycles of carboplatin plus pemetrexed at that time would have similar outcomes then. Would they have an improvement in those outcomes? That way, are we able to spare some patients from either amivantamab plus lazertinib or chemotherapy plus osimertinib and still have a role just for single-agent osimertinib in those patients.
References
- Cho BC, Lu S, Felip E, et al. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. N Engl J Med. 2024;391(16):1486-1498. doi:10.1056/NEJMoa2403614
- Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer Progressing on Platinum Chemotherapy: Initial Results From the CHRYSALIS Phase I Study. J Clin Oncol. 2021;39(30):3391-3402. doi:10.1200/JCO.21.00662
- FDA approves lazertinib with amivantamab-vmjw for non-small cell lung cancer.News release. FDA. August 19, 2024. https://shorturl.at/8yOXi
- Planchard D, Jänne PA, Cheng Y, et al. Osimertinib with or without chemotherapy in EGFR-mutated advanced NSCLC. N Engl J Med. 2023;389(21):1935-1948. doi:10.1056/NEJMoa2306434
- Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol. 2024;35(1):77-90. doi:10.1016/j.annonc.2023.10.117
- Leighl NB, Akamatsu H, Lim SM, et al. Subcutaneous amivantamab vs intravenous amivantamab, both in combination with lazertinib, in refractory EGFR-mutated, advanced non-small cell lung cancer (NSCLC): Primary results, including overall survival (OS), from the global, phase 3, randomized controlled PALOMA-3 trial. J Clin Oncol. 2024;42(17):LBA8505. doi:10.1200/JCO.2024.42.17_suppl.LBA8505
- Paz-Ares LG, Spira AI, Han JY, et al. 1269P Preventing infusion-related reactions with intravenous amivantamab: Updated results from SKIPPirr, a phase II study. Annal Oncol. 2024;35(2):S812. doi:10.1016/j.annonc.2024.08.1326
- Cho BC, Girard N, Sauder MB, et al. P3.12D.04 Enhanced vs standard dermatologic management with amivantamab-lazertinib in advanced NSCLC: phase 2 COCOON study. J Thorac Oncol. 2024. 1200-1400. doi.10.1016/j.jtho.2024.09.626










