(P040) Gastrointestinal Impact of Proton Radiation to the Spine in Pediatric Patients
Radiation to the spine may be associated with gastrointestinal (GI) toxicity, including nausea, vomiting, anorexia, and esophagitis. Proton therapy is expected to reduce this due to decreased exposure of the GI system when posterior-anterior beams are utilized.


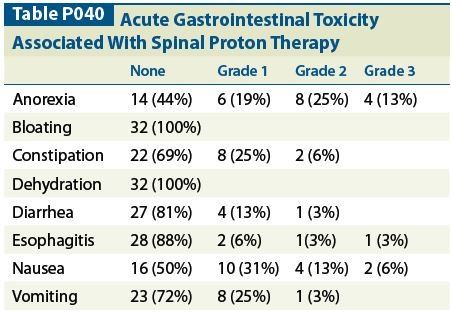
Table P040
Christine E. Hill-Kayser, MD, Stefan Both, PhD, Zelig Tochner, MD, Robert A. Lustig, MD; Perelman School of Medicine, University of Pennsylvania
Introduction: Radiation to the spine may be associated with gastrointestinal (GI) toxicity, including nausea, vomiting, anorexia, and esophagitis. Proton therapy is expected to reduce this due to decreased exposure of the GI system when posterior-anterior beams are utilized.
Methods: A consecutive series of 31 pediatric patients received proton therapy to the spine using posterior beams at the Children’s Hospital of Philadelphia/Roberts Proton Therapy Institute. Gastrointestinal dosimetry was evaluated at the time of radiation planning. Acute toxicities were evaluated weekly during proton therapy.
Results: A total of 32 patients (15 male) were evaluated; average age was 12 years (range: 2–20 yr). Of them, 25 received radiation to the total spine, and 6 received radiation to the partial spine (4 thoracic, 2 lumbar, 1 cervical). For those requiring total spine radiation, matchline changes were performed after each 900 cGy relative biological effectiveness (RBE). Proton radiotherapy dose ranged from 2,340 cGy (RBE) to 7,200 cGy (RBE), depending on clinical factors, and 19 patients received concurrent chemotherapy. Proton dosimetry to the esophagus, stomach, and bowel was evaluated at the time of radiation planning. Dose to the stomach and bowel was essentially 0 for all patients. Esophageal dose was very heterogeneous, with maximum ranging from near 0 to 6,180 cGy (RBE), and mean dose was < 1,000 cGy for all patients. Anorexia was the most common acute GI toxicity, affecting 16 patients (50%), followed by nausea (15, 47%) and constipation (10, 31%) (Table). The majority of GI effects were grade (G) 1 or 2, although four patients experienced G3 anorexia, one experienced G3 esophagitis, and one experienced G3 nausea. Dosimetry for the patient with G3 esophagitis demonstrated a maximum radiation dose of 2,120 cGy; however, the patient required daily intubation for anesthesia and also received chemotherapy concurrently. No patient experienced G4 acute GI toxicity.
Conclusions: Pediatric patients who were treated with proton therapy to the spine using posterior fields developed relatively mild acute toxicity, with > grade 2 acute toxicity rare. Some patients did experience bothersome anorexia and nausea. These side effects will continue to require support from the clinical team, despite improved dosimetry to the GI tract with use of proton radiotherapy.















