The Multidisciplinary Management of Paragangliomas of the Head and Neck, Part 1
Paragangliomas most commonly occur in the carotid body, jugulotympanicarea, and vagus nerve but have also been reported in otherareas of the head and neck. These tumors are highly vascular andcharacteristically have early blood vessel and neural involvement,making their treatment particularly challenging. Surgery has traditionallybeen the preferred method of treatment, especially in light of recentadvances in technique. However, compared to radiation therapy, it canresult in a higher incidence of cranial nerve dysfunction. Radiationtherapy has the advantage of avoiding the increased morbidity ofsurgery while offering an equal possibility of cure. Part 1 of this two-partarticle focuses on techniques for diagnosing paraganglioma and theindications for and use of surgery as primary treatment. The complicationscommonly associated with surgery are reviewed, and strategies forrehabilitation of affected patients are presented.
ABSTRACT: Paragangliomas most commonly occur in the carotid body, jugulotympanic area, and vagus nerve but have also been reported in other areas of the head and neck. These tumors are highly vascular and characteristically have early blood vessel and neural involvement, making their treatment particularly challenging. Surgery has traditionally been the preferred method of treatment, especially in light of recent advances in technique. However, compared to radiation therapy, it can result in a higher incidence of cranial nerve dysfunction. Radiation therapy has the advantage of avoiding the increased morbidity of surgery while offering an equal possibility of cure. Part 1 of this two-part article focuses on techniques for diagnosing paraganglioma and the indications for and use of surgery as primary treatment. The complications commonly associated with surgery are reviewed, and strategies for rehabilitation of affected patients are presented.
Paragangliomas are highly vascular neoplasms arising embryologically from the paraganglia of neural crest origin and occurring most commonly in the head and neck region. Typically, paragangliomas manifest in the 5th or 6th decade of life,[1,2] predominantly in females.[3-6] A slowly enlarging neck mass and/or findings consistent with cranial nerve dysfunction are the hallmarks of presentation.
Part 1 of this two-part article addresses the etiology and epidemiology of paragangliomas, their diagnosis, and surgical approaches to treatment. Part 2, which will appear in next month's issue, describes the use of radiation therapy in management and offers an overall treatment algorithm.
Overview
FIGURE 1


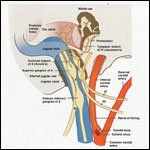
Paraganglioma Anatomy
Paraganglia are part of the diffuse neuroendocrine system, previously known as the amine precursor decarboxylate system, and have the potential to secrete neuropeptides and catecholamines.[7,8] Paragangliomas most commonly occur in the carotid body, jugulotympanic area, and vagal paraganglia (Figure 1), although they have also been reported in the larynx,[9] orbit,[10] thyroid,[ 11] tongue,[12] nasal cavity,[13] paranasal sinuses,[13,14] external auditory canal,[15] and supratentorial locations.[16,17]
Risk factors include high altitude and, in 5% to 10% of cases,[18,19] a hereditary predisposition characterized by autosomal dominant genetic transmission with variable penetration[ 20] and paternal imprinting.[ 20-22] Multicentric tumors are common in familial cases (78% to 87% have multiple paragangliomas)[ 6,19] but also occur in 10% of sporadic cases.[23] Such a presentation may result in refractory hypertension due to the loss of baroreceptive function after resection of bilateral carotid body tumors, whereas multiple tumors, including vagal or jugular paragangliomas, may result in multiple lower cranial nerve dysfunction.
Malignant paragangliomas are uncommon, and their diagnosis can only be confirmed by the presence of metastatic disease, usually within regional lymph nodes. There are no strict histologic criteria within the primary tumor to differentiate benign from malignant paragangliomas. Paragangliomas are highly vascular and characteristically associated with early involvement of blood vessels (carotid artery, jugular bulb) and neural areas (vagus, tympanic plexus), in addition to skull-base and potential intracranial extension.
These factors all contribute to the challenge of effectively treating these tumors. Traditionally, surgery has been the preferred method of treatment, especially with the evolution of more sophisticated skull-base approaches, safer embolization protocols, and advanced vascular bypass procedures.[24] Postoperative cranial nerve dysfunction is anticipated in patients with larger tumors and skullbase involvement, making rehabilitative efforts the focus of care.
Radiation therapy was traditionally used to treat unresectable paragangliomas or tumors in elderly or debilitated patients. Advances in radiation oncology and increased experience with the treatment of head and neck paragangliomas have led to improved long-term tumor responses with acceptable complications from radiation treatment. Radiation represents a reasonable primary treatment option especially for locally advanced or multicentric tumors, which, if surgically resected, would result in undue morbidity.
Incidence
TABLE 1



Distribution of Paragangliomas TABLE 2


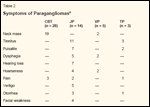
Symptoms of Paragangliomas TABLE 3


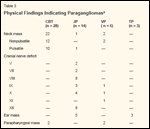
Physical Findings Indicating Paragangliomas
Paragangliomas of the head and neck are rare tumors, accounting for only 0.012% of all tumors reviewed by the surgical pathology department of Memorial Sloan-Kettering Cancer Center between 1938 and 1975.[25] The carotid body is the most common site of paragangliomas in the head and neck. Carotid body tumors, jugular paragangliomas, and tympanic paragangliomas account for 80% of all head and neck paragangliomas,[26] with vagal paragangliomas accounting for another 5%.[27] Nasal, orbital, laryngeal, and other paragangliomas occur much less frequently. Our review of 47 patients with 53 paragangliomas treated over a 10-year period (1990-2000) is consistent with the relative incidence of specific paragangliomas as reported by others (Tables 1-3).[28]
Malignant Variant
Malignant paragangliomas are uncommon. The most important criterion of malignancy is documented lymph node or distant metastases, as- the histologic examination of the primary tumor is unreliable in establishing a malignant diagnosis. The prevalence of malignancy depends on the site of the primary tumor. Among the more common types of head and neck paragangliomas, vagal paragangliomas most likely are associated with the highest rate of malignancy (about 10%),[29] with the regional lymph nodes and lungs being the most common sites of metastases.
Malignant carotid body tumors and jugulotympanic glomus tumors have been reported to occur in about 3% to 6% of cases.[30,31] Of head and neck paragangliomas, primary orbital and laryngeal tumors demonstrate the highest rate of malignancy (20% to 25% of cases).[23] The most common sites of distant carotid body tumor metastases are the bones, lungs, and liver,[32] while for jugulotympanic paragangliomas, the most common sites of metastases are the lungs, lymph nodes, liver, vertebrae, ribs, and spleen.[33]
In a review of 43 cases of malignant carotid body tumors, Pacheco- Ojeda[34] found that locoregional control requires resection of the pri- mary tumor and neck dissection followed by radiation therapy. The interval between primary resection and the appearance of a metastatic lesion may be long, ranging from 20 months to 20 years. Disseminated disease is relatively unresponsive to chemotherapy.
Growth Rate
Paragangliomas are slow-growing tumors with a mean growth rate of 1.0 mm/yr and a median doubling time of 4.2 years. Jansen et al reported less growth in very small and very large paragangliomas compared to intermediate- size tumors, suggesting a biphasic growth pattern.[35] The growth rate of metastases is slow, with a doubling time of 2,000 days.
Functioning Paragangliomas
Although all paragangliomas have the potential for releasing vasoactive substances such as catecholamines and dopamine,[29,36] only 1% to 3% produce associated clinical findings,[ 36,37] including excessive sweating, hypertension, tachycardia, nervousness, and weight loss.[36] Laboratory screening tests, including 24-hour urinary metanephrine (normal value < 1.3 mg) and vanillylmandelic acid levels (normal = 1.8-7.0 mg), are frequently elevated 10 to 15 times normal in patients with actively secreting tumors.[36]
Serum catecholamine levels, including serum norepinephrine and epinephrine, are also of value in the evaluation of patients. Because head and neck paragangliomas do not secrete epinephrine, an elevated serum epinephrine level is suggestive of a concurrent pheochromocytoma.[36] Several reports have noted an association between pheochromocytoma and both familial and nonfamilial paragangliomas.[ 38-40] Paragangliomas may occur in patients with both type IIA (pheochromocytoma, medullary thy- roid carcinoma, and parathyroid hyperplasia) and type IIB (also includes mucosal neuromas) familial multiple endocrine neoplasia.[41]
Diagnostic Evaluation
Computed Tomography
FIGURE 2



Carotid Body Tumor
Computed tomography (CT) with thin sections (1-3 mm) is an excellent imaging technique by which to identify paragangliomas and document the extent of tumor with precise evaluation of bone invasion. The classic CT findings of paragangliomas include a homogeneous mass with intense enhancement following administration of intravenous contrast (Figure 2). Although this appearance is typical of these tumors, it may also be seen with other vascular tumors such as neurolemmoma and meningioma.[24]
FIGURE 3



Vascular Involvement
Tumor location, displacement of major vessels, and patterns of involvement or invasion of surrounding structures aid in the diagnosis of paraganglioma. For example, carotid body tumors typically display the common carotid bifurcation with posterolateral displacement of the internal carotid artery (Figure 3A).[27] By contrast, vagal paragangliomas will displace both the internal and external carotid arteries anteriorly (Figure 3B), and are associated with erosion and widening of the jugular foramen.
Jugular paragangliomas may be distinguished from tympanic tumors based on early involvement of the skull base, erosion of the caroticojugular spine,[27,42] and destruction of the ossicular chain, which is unusual with tympanic tumors.[43]
Magnetic Resonance Imaging
FIGURE 4



T2-Weighted MRI Study With Gadolinium Contrast
Although CT is the study of choice for the evaluation of bone involvement, magnetic resonance imaging (MRI) provides meticulous soft-tissue detail and defines skull-base, intracranial, dural, and neural involvement, especially with the use of gadolinium enhancement (Figure 4).[28] Augmented by its ability to produce images in multiple planes, MRI is superior to CT in defining the relationship of paragangliomas to adjacent vascular and skull-base structures.
MRI studies of paragangliomas demonstrate a background tumor matrix of intermediate signal intensity on T1-and proton density-weighted images and moderately high signal intensity on T2-weighted images, along with scattered areas of focal signal voids, reflecting high-flow blood vessels.[44] Intense homogeneous contrast enhancement is seen.[44] On T2-weighted images, the classic MRI "salt and pepper" appearance, originally described by Olsen et al[45] and present in most lesions greater than 1.5 cm, reflects signal voids intermixed with regions of focally high signal intensity, the latter of which are probably due to sites of slow flow within the image plane (Figure 4).[44]
These findings, however, are not specific for paragangliomas, and may be seen with other hypervascular lesions (eg, metastasic renal cell carcinoma and thyroid carcinoma). That said, the typically smooth contour, sig- nal characteristics, and location of paragangliomas, coupled with a detailed clinical history and physical findings should result in an accurate diagnosis.
It is also worth noting that MRI is more effective than CT in identifying small synchronous paragangliomas, especially those smaller than 5 mm. (CT is most effective in demonstrating lesions greater than 8 mm.[46])
Magnetic resonance angiography (MRA) provides excellent visualization of the major head and neck vasculature and can demonstrate vessel displacement, gross tumor involvement, and possible compromised blood flow. It may be useful in defining flow-related enhancement of lesions greater than 1.5 cm.[27] While three-dimensional time-of-flight angiography appears superior to other MRA techniques in identifying some tumor feeders, its sensitivity is not high enough to demonstrate detailed tumor vascular supply, which is best defined by digital subtraction superselective angiography.[47]
Radioisotope Imaging
Paragangliomas, like other neuroendocrine tumors, have been found to have a high density of somatostatin type 2 receptors on their cell surface. Octreotide (Sandostatin) is a somatostatin analog, which, when coupled to the radioisotope indium-111, creates a scintigraphic image of tumors expressing somatostatin type 2 receptors. In a study of 21 patients with presumed head and neck paragangliomas who underwent indium-111/ octreotide scintigraphy, Telischi et al demonstrated an accuracy of 90%, a sensitivity of 94%, and a specificity of 75% in detecting tumors with this technique.[48]
Radioisotope scintigraphy provides a noninvasive imaging modality that is particularly useful in screening families with a history of paragangliomas. In addition, it is useful in detecting both synchronous and metachronous metastatic tumors.
Angiographic Evaluation
Angiography plays an important role in the evaluation of paragangliomas if surgery is being contemplated. It provides exquisite detail of the vascular anatomy, delineating the tumor blood supply (and possible anastomoses),[ 2] displacement of vessels, potential vessel compromise by tumor invasion, and adequacy of intracranial circulation if internal carotid artery sacrifice is necessary; this technique can also reveal previously undiagnosed synchronous paragangliomas.[ 49] Superselective angiography allows safe preoperative embolization of the tumor vasculature, hopefully avoiding proximal vessel occlusion and unexpected migration of embolization material into the cerebral or systemic circulation.
FIGURE 5



Contralateral Cerebral Blood Vessels
Our method of internal carotid balloon occlusion performed under local anesthesia with monitoring of mental functions for 20 minutes seems to be reliable in predicting a patient's tolerance to the interruption of carotid blood flow. More recently, we have relied on angiographic evidence of adequate contralateral cerebral blood without performing elective internal carotid balloon occlusion (Figure 5).
In our study of 28 patients undergoing cerebral angiography, 26 (93%) demonstrated angiographic or balloon occlusion testing evidence of tolerance to possible carotid sacrifice.[ 28] With this preoperative information, surgical decisions about carotid bypass options can be made. Even with preparation for internal carotid artery grafting, a review of multiple series reports a 9.7% rate of strokes and a 2.4% incidence of mortality.[50]
TABLE 4



Commonly Used Staging Systems for Carotid Body Tumors and Jugulotympanic Paragangliomas
In our series, 4 of 47 patients with previously undiscovered paragangliomas were diagnosed on angiography (three carotid body tumors, one vagal paraganglioma). For these reasons, bilateral carotid angiography is an important part of the protocol in our evaluation of patients who are to undergo surgery.[28]
Biopsy
If a diagnosis of paraganglioma is suspected, an incisional biopsy is contraindicated due to the risk of hemorrhage and subsequent fibrosis at the operative site.[51] A fineneedle aspiration biopsy may be performed safely with minimal risk of bleeding.
Staging
The most commonly used staging systems for carotid body tumors and jugulotympanic paragangliomas are listed in Table 4.
Management Options
Traditionally, surgical resection has been the mainstay of treatment for these tumors, but the outcome is dependent on many factors that may influence the ideal result of total tumor removal and minimal postoperative complications. Relative contraindications to surgery include extensive skull-base or intracranial involvement, advanced age of the patient, medical comorbidities, and bilateral or multiple paragangliomas, which may result in unacceptable postoperative morbidity and bilateral lower cranial nerve palsies.
If surgery is the chosen course of treatment, preoperative embolization is performed. Embolization of paragangliomas has been an extremely useful adjunct to our treatment protocol. Although not uniformly accepted,[ 52-56] there are major advantages to performing endovascular embolization prior to subsequent surgery, assuming that certain criteria have been met before the embolization is performed.[41,57-61] An experienced vascular radiology team must be thoroughly familiar with the complexities and possible variations in the vascular anatomy of the head and neck. Many anastomoses exist between the external and internal carotid system, and without this knowledge, disastrous neurologic consequences may result.[62] The safe performance of this procedure by interventional vascular radiology must be established and documented with an acceptable rate of morbidity and mortality.[60,63]
Surgery
Surgery is performed within 2 days of angiography and embolization to avoid recruitment of collateral tumor blood supply and prior to the onset of a significant postinflammatory effect.[ 28] If there is concern about tumor edema, which may compromise the dissection, short-term steroids are administered. The anesthesiologist must be prepared to counteract the alpha- and beta-adrenergic catecholamine- induced cardiovascular effect when dealing with "secreting" tumors.
Carotid Body Tumors
Adequate removal of the tumor requires a subadventitial dissection of the carotid artery. Nerves adherent to but not infiltrated by these tumors can usually be mobilized; these include the vagus, hypoglossal, and, occasionally, glossopharyngeal nerves. The sympathetic chain and the superior laryngeal nerve are often adherent to tumor, especially in cases with medial extension into the parapharyngeal space.
Jugulotympanic Paragangliomas
Tympanic paragangliomas confined to the middle ear (Glasscock- Jackson type I, Fisch class A) can be accessed via a transcanal approach.[ 64] These small tumors do not require preoperative embolization.
Involvement of the jugular bulb requires a combined transmastoid and transcervical approach.[65] Tumor dissection is meticulously performed off the internal carotid artery. The exiting cranial nerves are preserved if they can be adequately separated from the tumor. Additional exposure into the infratemporal fossa can be accomplished with resection of the mandibular condyle and zygomatic arch. Such an approach allows access to the posterior and middle cranial fossa, and, if necessary, further tumor resection can be accomplished through a neurosurgical, intracranial approach. A pedicled temporalis, temporal- parietal, or sternomastoid flap is used to reconstruct and obliterate the defect. The external auditory canal is closed at the meatus. Spinal drainage catheters are used postoperatively for significant cerebrospinal fluid leaks.
Vagal Paragangliomas
Vagal paragangliomas may vary in the extent of skull-base or intracranial involvement. Most vagal paragangliomas originate in the nodose (inferior) ganglion, approximately 2 cm below the jugular foramen. When these tumors grow, they will extend to the skull base and involve the post styloid parapharyngeal space as well. Vagal paragangliomas arising in the middle or superior vagal ganglia are associated with early skull-base involvement with intracranial extension.
As with all paragangliomas, a complete radiographic evaluation with contrast-enhanced MRI and CT stud- ies will define the extent of involvement. A combined cervical-mastoid approach to the skull base is best for achieving safe and wide exposure. The tumor almost always involves sacrifice of the vagus nerve and additional cranial nerves according to its size and local involvement.[6]
Complications
The complications associated with head and paraganglioma surgery can be grouped into three main categories: cranial nerve injury, vascular injury, and injury to the carotid body/ carotid sinus complex.
Cranial Nerve Injury
Lower cranial nerve dysfunction is a common complication of surgical resection of head and neck paragangliomas and often requires postoperative rehabilitation.[6] Indeed, larger tumors that involve the temporal bone can infiltrate between the fascicles of the cranial nerves, even with normal nerve function. These involved nerves should be sacrificed to effect a total tumor resection.[66] Our experience with postoperative cranial nerve dysfunction reflects a combination of total paralysis, due to nerve sacrifice and paresis, with ultimate recovery of function due to nerve traction.
TABLE 5


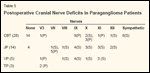
Postoperative Cranial Nerve Deficits in Paraganglioma Patients
The frequency of affected nerves is related to tumor type and size and the surgical approach used (Table 5).[28] Although isolated injury to one of the lower cranial nerves (IX-XII) sometimes causes only temporary minor difficulty in swallowing, aspiration, phonation, shoulder mobility, or tongue motion, vagus nerve and multiple cranial nerve injury may result in significant morbidity.[ 67] Multiple cranial nerve deficits are particularly poorly tolerated by elderly patients. Bilateral lower cranial nerve palsies most often represent a severe, potentially life-threatening situation.
Postoperative Rehabilitation
Paraganglioma surgery generally produces postoperative nerve dysfunction, and familiarity with rehabilita tion techniques is necessary for proper patient care. If tumor resection results in nerve transection, then primary anastomosis, if possible, results in acceptable function. This is especially true of the facial, accessory, and hypoglossal nerves. Cable grafts using the greater auricular or sural nerve are also an option, especially in the case of facial and accessory nerve dysfunction.
Rehabilitation for patients with postoperative nerve dysfunction depends on the functional deficit and may require additional surgical intervention, including upper-lid gold-weight implants for corneal protection, transoral hemipalatal adhesion for palatal insufficiency,[68] temporalis and masseter muscle/ fascial sling or adynamic fascial or allograft slings for facial muscle weakness, and gelatin (Gelfoam) injection/ silastic implant of a paralyzed vocal cord for medialization to potentiate swallowing and improve voice quality.
Vascular Injury
The incidence of intraoperative or postoperative stroke has decreased dramatically as surgical and anesthetic techniques have improved. This improvement has been attributed to many factors, including detailed preoperative imaging and angiographic evaluation to determine vessel involvement by tumor, carotid occlusion testing, correlation of bilateral cerebral angiography findings with postocclusion cerebral function, and advances in surgical arterial revascularization techniques. Recent series report a 0% to 2% rate of major strokes as a complication of carotid body tumor resection[ 1,50,55,69-72]; earlier series reported a rate of 10% to 20%.[72,73]
REFERENCE GUIDE
Therapeutic Agents
Mentioned in This Article
Clonidine
Phenoxybenzamine (Dibenzyline)
Sodium nitroprusside
Brand names are listed in parentheses only if a drug is not available generically and is marketed as no more than two trademarked or registered products. More familiar alternative generic designations may also be included parenthetically.
Compared to carotid body paragangliomas, vagal paragangliomas are usually not as intimately associated with the great vessels, making vascular injury less likely.[74] Netterville et al reported carotid artery encasement in 5 of 46 patients with vagal paragangliomas.[6] Other paragangliomas associated with vascular injury include large jugular paragangliomas, which commonly involve the internal carotid artery, especially if there is erosion of the bony partition between the internal jugular vein and the internal carotid artery. Internal carotid artery damage occurred in only 1% of patients with large paragangliomas of the skull base.[75]
Carotid Body/Carotid Sinus Complex
Resection of bilateral carotid body tumors can result in baroreceptive dysfunction due to bilateral denervation of the carotid sinus. This dysfunction manifests as sustained hypertension and tachycardia. Netterville et al reported that 10 of 11 patients who underwent bilateral carotid sinus denervation demonstrated severe labile hypertension/hypotension, headache, diaphoresis, and emotional instability.[19]
As the parasympathetic response is lost, unopposed sympathetic stimuli result in cardiovascular morbidity, which is usually successfully managed postoperatively with alphaadrenergic antagonists. Sodium nitroprusside is administered in the early postoperative period to prevent hypertension. The long-term cardiovascular effects are controlled with clonidine or phenoxybenzamine (Dibenzyline).
Financial Disclosure:The authors have no significant financial interest or other relationship with the manufacturers of any products or providers of any service mentioned in this article.
References:
1.
Williams MD, Phillips MJ, Nelson WK,et al: Carotid body tumor. Arch Surg 127:963-968, 1992.B
2.
Gaylis H, Davidge-Pitts K, PantanowitzD: Carotid body tumours. A review of 52cases. S Afr J Surg 72:493-496, 1987.
3.
Jackson CG, Harris PF, Glassock ME 3rd,et al: Diagnosis and management of paragangliomasof the skull base. Am J Surg 159:389-393, 1990.
4.
Lawson W: Glomus bodies and tumors. NY State J Med 80:1567-1575, 1980.
5.
Moore G, Yarington CT Jr, Mangham CAJr: Vagal body tumors: Diagnosis and treatment.Laryngoscope 96:533-536, 1986.
6.
Netterville JL, Jackson CG, Miller FR, etal: Vagal paraganglioma: A review of 46 patientstreated during a 20-year period. ArchOtolaryngol Head Neck Surg 124:1133-1140,1998.
7.
Pearse A: The cytochemistry and ultrastructureof the polypeptide hormone-producingcells of the APUD series and the embryonic,physiologic and pathologic implications of theconcept. J Histochem Cytochem 17:303-313,1969.
8.
Pearse A: The diffuse neuroendocrine system:Historical review. Front Horm Res 12:1-7, 1984.
9.
Thirlwall AS, Bailey CM, Ramsay AD, etal: Laryngeal paraganglioma in a five-year-oldchild-the youngest case ever recorded. JLaryngol Otol 113:62-64, 1999.
10.
Venkataramana NK, Kolluri VR, KumarDV, et al: Paraganglioma of the orbit with extensionto the middle cranial fossa: A casereport. Neurosurgery 24:762-764, 1989.
11
. Kronz JD, Argani P, Udelsman R, et al:Paraganglioma of the thyroid: Two cases thatclarify and expand the clinical spectrum. HeadNeck 22:621-625, 2000.
12.
Nielsen TO, Sejean G, Onerheim RM:Paraganglioma of the tongue. Arch Pathol LabMed 124:877-879, 2000.
Paraganglioma of the tongue. Arch Pathol LabMed 124:877-879, 2000.
13.
Welkoborsky HJ, Gosepath J, Jacob R,et al: Biologic characteristics of paragangliomasof the nasal cavity and paranasal sinuses. AmJ Rhinol 14:419-426, 2000.
14.
Sharma HS, et al: Malignant paragangliomaof frontoethmoidal region. Auris NasusLarynx 26:487-493, 1999.
15.
Skinner LJ, Curran AJ, Barnes C, et al:Paraganglioma of the external auditory canal:An unusual case. J Laryngol Otol 114:370-372, 2000.
16.
Sambaziotis D, Kontogeroges G, KovacsK, et al: Intrasellar paraganglioma presentingas nonfunctioning pituitary adenoma.Arch Pathol Lab Med 123:429-432, 1999.
17
. Yamauchi T, Kubota M, Saeki N, et al:Paraganglioma in the frontal skull base-casereport. Neurol Med Chir 39:308-312, 1999.
18.
Grufferman S, Gillman MW, PasternakLR, et al: Familial carotid body tumors: Casereport and epidemiologic review. Cancer46:2116-2122, 1980.
19.
Netterville JL, ReillyKM, Robertson D,et al: Carotid body tumors: A review of 30patients with 46 tumors. Laryngoscope 105:115-126, 1995.
20.
Oosterwijk J, Jansen JC, van SchothorstEM, et al: First experience with genetic counsellingbased on predictive DNA diagnosis inhereditary glomus tumors (paragangliomas). JMed Genet 33:379-383, 1996.
21.
van der Mey AG, Maaswinkel-MooyPD, Cornelissa CJ, et al: Gentic imprinting inhereditary glomus tumours: Evidence for a newgenetic theory. Lancet 2:1291-1894, 1989.
22.
Heutink P, van der Mey AG, SankuijlLA, et al: A gene subject to genomic imprintingand responsible for hereditary paragangliomasmaps to chromosome 11q23-qter. HumMol Genet 1:7-10, 1992.
23.
Sykes J, Ossoff R: Paragangliomas ofthe head and neck. Otolaryngol Clin North Am19:755-767, 1986.
24.
Jackson G: Diagnosis for treatment planningand treatment options. Laryngoscope103:17-22, 1993.
25.
Lack EF, Cubilla AL, Woodruff JM, etal: Paragangliomas of the head and neck region:A clinical study of 69 patients. Cancer39:397-409, 1977.
26.
Kliewer KE, Wen DR, Cancilla PA, etal: Paragangliomas: Assessment of prognosisby histologic, immunohistochemical, and ultrastructuraltechniques. Hum Pathol 20:29-39,1989.
27.
Rao AB, Koeller KK, Adair CF: Fromthe archives of the AFIP. Paragangliomas ofthe head and neck: Radiologic-pathologic correlation.Armed Forces Institute of Pathology.Radiographics 19:1605-1632, 1999.
28.
Persky MS, Setton A, Niimi Y, et al:Combined endovascular and surgical treatmentof head and neck paragangliomas-A team approach.Head Neck 24:423-431, 2002.
29.
Batsakis J: Paragangliomas of the headand neck, in Tumors of the Head and Neck:Clinical and Pathological Consideration,pp 369-380. Baltimore, Williams & Wilkins,1979.
30.
Shamblin WR, Mine WH, Sheps SG, etal: Carotid body tumor (chemodectoma): Clinicopathologicanalysis of ninety cases. Am Surg122:732-739, 1971.
31.
Manolidis S, Shohet JA, Jackson CG, etal: Malignant glomus tumors. Laryngoscope109:30-34, 1999.
32.
Zbaren P, Lehman W: Carotid bodyparaganglioma with metastasis. Laryngoscope95:450-454, 1985.
33.
El Fiky FM, Paparella MM: A metastaticglomus jugulare tumor. A temporal bonereport. Am J Otol 5:197-200, 1984.
34.
Pacheco-Ojeda L: Malignant carotid bodytumors: Report of three cases. Ann Otol RhinolLaryngol 110:36-40, 2001.
35.
Jansen JC, van den Berg R, Kuiper A, etal: Estimation of growth rate in patients withhead and neck paragangliomas influences thetreatment proposal. Cancer 88:2811-2816, 2000.
36.
Schwaber MK, Glasscock ME, NissenAJ, et al: Diagnosis and management of catecholaminesecreting glomus tumors. Laryngoscope94:1008-1015, 1984.
37.
Zak FG, Lawson W: The ParaganglionicChemoreceptor System. New York, Springer-Verlag, 1982.
38.
Irons GB, Weiland LH, Brown WL:Paragangliomas of the neck: Clinical and pathologicanalysis of 116 cases. Surg Clin NorthAm 57:575-583, 1977.
39.
Parkin JL: Familial multiple glomus tumorsand pheochromocytomas. Ann Otol RhinolLaryngol 90:60-63, 1981.
40.
Revak CS, Morris SE, Alexander GH:Pheochromocytoma and recurrent chemodectomasover a twenty-five year period. Radiology100:53-54, 1971.
41.
Maier W, Marangos N, Laszig R: Paragangliomaas a systemic syndrome: Pitfalls and strategies.J Laryngol Otol 113:978-982, 1999.
42.
Cheng A, Niparko JK: Imaging quizcase 2. Glomus tympanicum tumor of the temporalbone. Arch Otolaryngol Head Neck Surg123:549, 551-552, 1997.
43.
Swartz JD, Harnsberger HR, MukherjiSK: The temporal bone. Contemporary diagnosticdilemma. Radiol Clin North Am 36:819-853, 1998.
44.
Som PM, Braun IF, Shapiro MD, et al:Tumors of the parapharyngeal space and upperneck: MR imaging characteristics. Radiology164:823-829, 1987.
45.
Olsen WL, Dillon WP, Kelly WM, et al:MR imaging of paragangliomas. AJR Am JRoentgenol 148:201-204, 1987.
46.
van Gils AP, van der May AG, HoogmaRP, et al: MRI screening of kindred at risk ofdeveloping paragangliomas: Support for genomicimprinting in hereditary glomus tumours.Br J Cancer 65:903-907, 1992.
47.
van den Berg R, Wasser MN, van GilsAP, et al: Vascularization of head and neckparagangliomas: Comparison of three MR angiographictechniques with digital subtractionangiography. Am J Neuroradiol 21:162-170,2000.
48.
Telischi FF, Bustillo A, Whiteman ML,et al: Octreotide scintigraphy for the detectionof paragangliomas. Otolaryngol Head NeckSurg 122:358-362, 2000.
49.
Lasjaunias AP, Berenstein K: SurgicalNeuro-angiography: Endovascular Treatmentof Craniofacial Lesions, vol 2. New York,Springer-Verlag, 1987.
50.
Anand VK, Alemar GO, Sanders TS:Management of the internal carotid artery duringcarotid body tumor surgery. Laryngoscope105(3 pt 1):231-235, 1995.
51.
Sakurai H, Hayakawa K, Mitsuhashi N,et al: Chemodectoma of the carotid body treatedwith radiation therapy: A case report. RadiatMed 13:191-194, 1995.
52.
Biller H, Lawson W, Som P, et al: Glomusvagale tumors. Ann Otol Rhinol Laryngol98(1 pt 1):21-26, 1989.
53.
Brackman D, Kinney S, Fu K: Glomustumor: Diagnosis and management. Head NeckSurg 9:306-311, 1987.
54.
Leonetti JP, Donzelli JJ, Littooy FN, etal: Perioperative strategies in the managementof carotid body tumors. Otolaryngol Head NeckSurg 117:111-115, 1997.
55.
Matticari S, Credi G, Pratesi G, et al:Diagnosis and surgical treatment of the carotidbody tumors. J Cardiovasc Surg 36:233-239,1995.
56.
Litle VR, Reilly LM, Ramos TK: Preoperativeembolization of carotid body tumors:When is it appropriate? Ann Vasc Surg 10:464-468, 1996.
57.
Merland JJ, Reizine D, Guimaraens L, etal: Diagnostic and therapeutic angiography inthe evaluation and treatment of glomus jugularetumors. Apropos of 32 cases (French). Neuro-Chirurgie 31:358-366, 1985.
58.
Ogura JH, Spector GJ, Gado M: Glomusjugulare and vagale. Ann Otol 87(5 pt 1):622-629, 1978.
59.
Smith RF, Shetty PC, Reddy DJ: Surgicaltreatment of carotid paragangliomas presentingunusual technical difficulties. The valueof preoperative embolization. J Vasc Surg7:631-637, 1988.
60.
LaMuraglia GM, Fabian RL, BrewsterDC, et al: The current surgical management ofcarotid body paragangliomas. J Vasc Surg15:1038-1045 (incl discussion), 1992.
61.
Ward PH, Liu C, Vinuela F, et al: Embolization:An adjunctive measure for removal ofcarotid body tumors. Laryngoscope 98:1287-1291, 1988.
62.
Lasjaunias P: Nasopharyngeal angiofibromas:Hazards of embolization. Radiology136:119-123, 1980.
63
. Murphy TP, Brackmann DE: Effects ofpreoperative embolization on glomus jugularetumors. Laryngoscope 99:1244-1247, 1989.
64.
House WF, Glasscock ME: Glomus tympanicumtumors. Arch Otolaryngol 87:550,1968.
65.
Brackmann D, Arriaga M: Surgery forglomus tumors, in Brackmann D, Shelton C,Arriaga M (eds): Otologic Surgery. Philadelphia,WB Saunders, 1994.
66.
Sen C, Hague K, Kacchera R, et al:Jugular foramen: Microscopic anatomic featuresand implications for neural preservationwith reference to glomus tumors involving thetemporal bone. Neurosurgery 48:838-848,2001.
67.
Jackson CG: Skull base surgery. Am JOtol 3:161-171, 1981.
68.
Netterville JL, Vrabec JT: Unilateral palataladhesion for paralysis after high vagalinjury. Arch Otolaryngol Head Neck Surg120:218-221, 1994.
69.
Dickinson PH, Griffin SM, Guy AJ, etal: Carotid body tumour: 30 years experience.Br J Surg 73:14-16, 1986.
70.
Hallett JW Jr, Nora JD, Hollier LH, et al:Trends in neurovascular complications of surgicalmanagement for carotid body and cervicalparagangliomas: A fifty-year experiencewith 153 tumors. J Vasc Surg 7:284-291,1988.
71.
Wax MK, Briant TD: Carotid body tumors:A review. J Otolaryngol 21:277-285,1992.
72.
Muhm M, Polterauer P, Gstottner W, etal: Diagnostic and therapeutic approaches tocarotid body tumors. Review of 24 patients.Arch Surg 132:279-284, 1997.
73.
Monro R: The natural history of carotidbody tumours and their diagnosis and treatment.Br J Surg 37:4445-453, 1950.
74.
Urquhart AC, Johnson JT, Myers EN, etal: Glomus vagale: Paraganglioma of the vagusnerve. Laryngoscope 104:440-445, 1994.
75.
Woods CI, Strasnick B, Jackson CG:Surgery for glomus tumors: The Otology Groupexperience. Laryngoscope 103:65-70, 1993.













