(P130) Implication of Treatment Approach Based on Histology of Thymic Tumors
Thymic tumors are a rare disease and have been treated in a similar manner without convincing data. We present our institutional results of outcomes between invasive thymoma and thymic carcinoma.


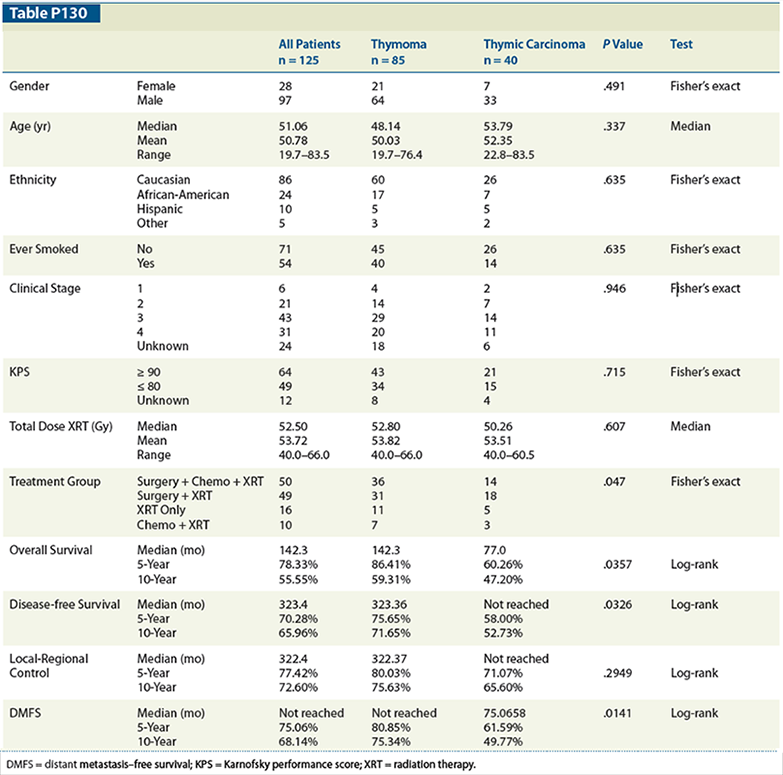
Table P130
Komaki Ritsuko, MD, Xiong Wei, MD, Daniel Gomez, MD, Osamu Takahashi, MD, Pamela Allen, PhD, James D. Cox, MD; UT MD Anderson Cancer Center
Background: Thymic tumors are a rare disease and have been treated in a similar manner without convincing data. We present our institutional results of outcomes between invasive thymoma and thymic carcinoma.
Materials and Methods: Between 1964 and 2009, 125 patients with thymoma (85) or thymic carcinoma (40) were treated at UT MD Anderson Cancer Center. Treatments were follows: 50 patients (induction chemotherapy + surgery + postoperative XRT), 49 patients (surgery + radiation therapy), 16 patients (radiation only), and 10 patients (chemotherapy + XRT). The data were analyzed using Kaplan-Meier survival function. The log-rank test was used to assess survival function. Cox regression analysis was used for univariate and multivariate analysis.
Results: The median follow-up for invasive thymoma and thymic carcinoma was 79 and 46 months, respectively. Age, ethnicity, smoking history, clinical staging, Karnofsky performance score (KPS), and total dose of radiotherapy were not significantly different between the two groups. All clinical stage I or II patients, except for one inoperable patient, were found to have Masaoka stage III disease and received combined treatment. Five-year and 10-year survival rates were significantly better for the thymoma group compared with the thymic carcinoma group. Overall survival (OS) was 86% vs 60% and 59% vs 47%, respectively (P = .04). Disease-free survival (DFS) was 76% vs 58% and 72% vs 53%, respectively (P = .0326). Distant metastasis-free survival (DMFS) was 81% vs 62% and 75% vs 50%, respectively (P = .0141). Multivariate analysis showed that histology, clinical stage, and KPS were significant prognostic factors for predicting OS. Histology, ethnicity, and age were significantly correlated with DM.
Conclusions: Thymic carcinoma patients showed significantly poor OS, DFS, and DMFS compared with thymoma patients. We need to investigate more adequate systemic chemotherapy for thymic carcinoma rather than standard chemotherapy used for invasive thymoma.















