Proposed Algorithm for Managing Ibrutinib-Related Atrial Fibrillation
Although ibrutinib-related atrial fibrillation (IRAF) occurs in up to 11% of patients in clinical trials, these studies have rarely fully characterized bleeding events or risk factors for bleeding when ibrutinib is combined with anticoagulation. Furthermore, guidelines do not provide direction regarding the preferred anti-arrhythmic agent for IRAF.


Oncology (Williston Park). 30(11):970–981, C3.


Table 1. Bleeding and Atrial Fibrillation Events Reported in Clinical Trials
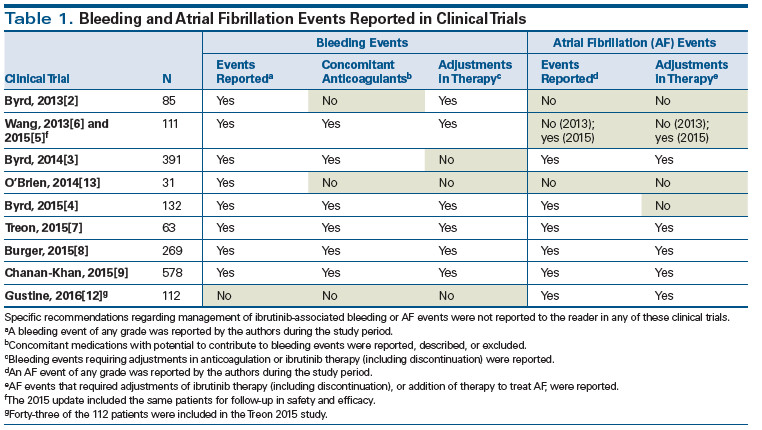


Table 2. CHA2DS2-VASc Scoring
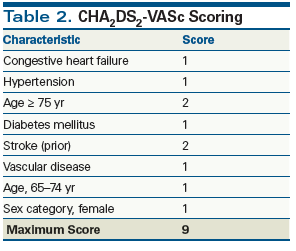


Table 3. Recommended Anticoagulation Therapy
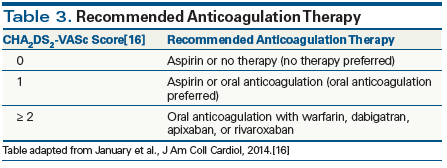


Table 4. CHA2DS2-VASc Score and Adjusted Stroke Rate
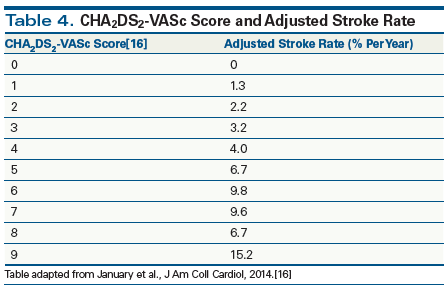


Table 5. HAS-BLED Scoring
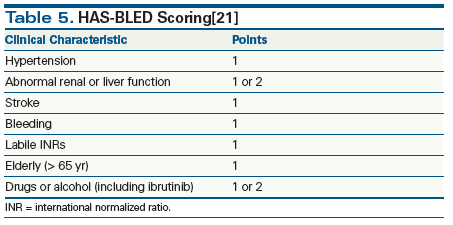


Table 6. HAS-BLED Score and Bleeding Risk
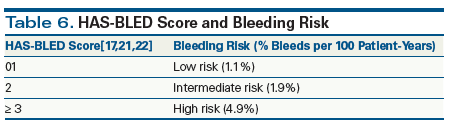


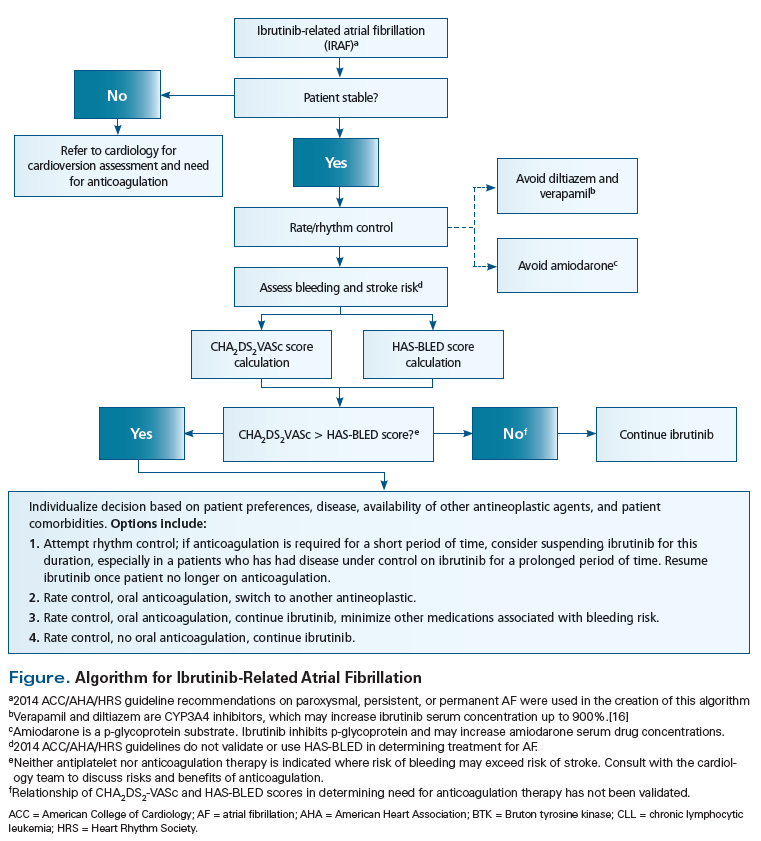
Figure. Algorithm for Ibrutinib-Related Atrial Fibrillation
Introduction
Ibrutinib, an oral small molecule inhibitor of Bruton tyrosine kinase (BTK), is approved for all patients with chronic lymphocytic leukemia (CLL) and Waldenström macroglobulinema (WM) and as a second-line agent for patients with mantle cell lymphoma (MCL).[1] Ibrutinib selectively and irreversibly inhibits BTK within B lymphocytes to block constitutively activated intracellular signaling pathways that are critical to cell migration and survival.
Ibrutinib is generally well tolerated but, importantly, possesses off-target effects. Two adverse events increasingly recognized from clinical trials and clinical experience are bleeding and atrial fibrillation (AF).[2-9] In vitro, ibrutinib has been shown to inhibit BTK and Tec kinase, leading to inhibition of glycoprotein VI (GPVI)- and GP1b-mediated platelet function, and a subsequent inhibition of platelet aggregation, resulting in decreased platelet adhesion to von Willebrand factor.[10] The mechanism of ibrutinib-related atrial fibrillation (IRAF) is more elusive. A preclinical mouse model suggested that AF may be induced by inhibition of phosphoinositide 3-kinase (PI3K) p110α (another important member of the B-cell receptor signaling pathway) in cardiac myocytes. However, this is highly debated and still unclear.[11] Managing AF in patients receiving ibrutinib is particularly challenging, given that to date the natural course of this adverse event cannot be predicted. Anticoagulation is indicated in a significant proportion of patients with AF, with the goal of decreasing the risk of thromboembolic complications. However, since bleeding is a common side effect of ibrutinib, the feasibility of using anticoagulation to prevent thrombotic stroke, while simultaneously avoiding hemorrhagic stroke, requires further study and discussion.
Although IRAF occurs in up to 11% of patients in clinical trials, these studies have rarely fully characterized bleeding events or risk factors for bleeding when ibrutinib is combined with anticoagulation.[2-9,12,13] Furthermore, guidelines do not provide direction regarding the preferred anti-arrhythmic agent for IRAF. As ibrutinib continues to gain momentum against a large spectrum of B-cell malignancies, developing guidance for the management of IRAF is of the utmost importance. The bleeding risk can be severe and must not be ignored.[3,14] Therefore, we have three goals in presenting the information in this article:
1) To describe the frequency of IRAF and subsequent bleeding events reported in clinical trials.
2) To introduce the concept of using CHA2DS2-VASc and HAS-BLED scoring methods to characterize venous thromboembolism risk and bleeding risk, respectively, when considering anticoagulation for IRAF.
3) To propose an algorithm for the management of IRAF that weighs the risks and benefits of combining ibrutinib with specific anticoagulants or antiarrhythmic medications.
IRAF Frequency and Subsequent Bleeding Events Reported in Clinical Trials
To identify clinical trials that quantified the frequency and grade of bleeding as well as AF events associated with ibrutinib therapy, the following search terms were entered into the PubMed database, paired with “ibrutinib”: “chronic lymphocytic leukemia,” “mantle cell lymphoma,” “Waldenström macroglobulinema,” “atrial fibrillation,” “anticoagulation,” “stroke,” “venous thromboembolism,” “thrombosis,” “mechanism,” and “bleeding.” Search results revealed seven prospective, randomized clinical trials that assessed frequency of bleeding and AF events (Table 1).
In 2013, in a phase Ib/II trial, Byrd and colleagues compared the safety and efficacy of ibrutinib administered at a dose of 420 mg or 840 mg daily in 85 patients with relapsed or refractory CLL or small lymphocytic lymphoma (SLL).[2] Four patients experienced bleeding events of grade 3 or higher during the study period, but these events were not described. The authors reported ecchymoses and petechiae in a subgroup of patients who received ibrutinib, but they did not quantify these events. Ibrutinib therapy was discontinued in 1 patient who experienced gastrointestinal hemorrhage. The authors did not report or address AF events.
In 2013, Wang and colleagues published a phase II study using ibrutinib, 560 mg daily, in 111 patients with relapsed or refractory MCL.[6] Grade 1 and 2 contusions occurred in 19 patients. Five patients experienced grade 3 bleeding events, and 4 patients experienced subdural hematomas (varying from grade 1 to grade 3) due to falls or head trauma during the study period. It is unknown whether the 4 patients with subdural hematomas were taking aspirin or warfarin at the time of injury. The authors did not report or discuss the occurrence of AF. In 2015, Wang and colleagues published long-term safety and efficacy data in the same cohort of patients with relapsed or refractory MCL.[5] Bleeding events of any grade occurred in 50% of patients during the study period. The most frequent bleeding events included grade 1, 2, and 3 bruising (18%), epistaxis (11%), and petechiae (10%). It is unknown how many of the patients in whom these occurred were taking aspirin or warfarin at the time of injury. Initially, the use of concomitant warfarin was not restricted; however, amendments were made during the study period to restrict concomitant use of warfarin as a precaution. Ibrutinib was discontinued due to subdural hematomas in 2 patients. AF occurred in 12 patients (11%), 7 of whom experienced grade 3 events. Of note, 10 of the 12 patients who developed AF had a medical history significant for cardiovascular disease. Treatment of AF included beta-blockers, anti-arrhythmics (amiodarone or dronedarone), or ablation therapy. Six of the 12 patients with an AF event were anticoagulated with low-dose heparin or warfarin. There were no AF events that led to discontinuation of ibrutinib therapy.
In 2014, Byrd and colleagues published a phase III trial comparing the efficacy of ibrutinib vs ofatumumab in relapsed or refractory CLL or SLL in 391 patients.[3] Bleeding events of any grade were observed more frequently in the ibrutinib group (44%) compared with the ofatumumab group (12%). Major hemorrhage requiring transfusion of red cells or hospitalization was reported in 2 patients in the ibrutinib group vs 3 patients in the ofatumumab group. Patients requiring warfarin were excluded from this study. AF of any grade occurred in 10 patients (5%) in the ibrutinib group (n = 195), which led to the discontinuation of ibrutinib in 1 patient.
In 2014, O’Brien and colleagues conducted an open-label phase Ib/II safety trial comparing 420 mg vs 840 mg of ibrutinib as initial therapy for CLL and SLL in 31 elderly patients.[13] The authors reported the discontinuation of ibrutinib at 840 mg during enrollment because available data showed comparable efficacy for the 420-mg dose. The authors observed grade 1 epistaxis in 5 patients (16%) and petechiae in 5 patients (16%). The authors did not report or address AF occurrence.
In 2015, Byrd and colleagues published a 3-year follow-up report assessing the long-term safety of 420 mg or 840 mg of ibrutinib in 132 patients with symptomatic treatment-naive or relapsed/refractory CLL or SLL.[4] Any-grade bleeding events occurred in 61% of the cohort, with bruising and petechiae as the two most common events reported. During the 3-year follow-up period, major hemorrhage occurred in 10 patients. Ibrutinib therapy was discontinued in 3 patients (2.7%) due to subdural hematoma or gastrointestinal hemorrhage. The authors reported percentages of concomitant use of anticoagulants among the entire cohort of patients. These included: aspirin, 80%; antiplatelet agents, 58%; and anticoagulant agents, 22%. Originally, the authors did not enforce restrictions on the use of concomitant warfarin and ibrutinib; however, after review of warfarin-related bleeding events, protocol amendments were made to restrict the use of warfarin. During the follow-up period, the authors implemented guidelines for pre- and postoperative ibrutinib management to prevent bleeding events. During the follow-up period, 6% of patients in the entire patient cohort experienced AF.
In 2015, Treon and colleagues conducted a prospective study in 63 WM patients using ibrutinib, at 20-mg daily.[7] Bleeding events greater than grade 2 occurred in 4 patients (6.3%) and were described as epistaxis and postprocedural bleeding. The authors noted that concomitant fish-oil supplements were thought to have contributed to two of these bleeding events and were discontinued, with subsequent resolution of ibrutinib therapy–associated bleeding. An amendment to the study protocol recommended that ibrutinib be withheld for 3 to 7 days before and for 1 to 3 days after an invasive procedure. These guidelines were similar to those implemented in the 2015 long-term follow-up study by Byrd and colleagues. Patients receiving warfarin were excluded from the study. AF occurred in 3 patients (5%) with a history of arrhythmias. Ibrutinib was held in these patients, with no cardiologic intervention. When AF resolved, ibrutinib was resumed without complications in all 3 patients. Patients were excluded if they were taking medications with potential to prolong the QT interval, or if they had clinically significant cardiovascular disease.
In 2015, Burger and colleagues conducted a randomized phase III trial comparing ibrutinib with chlorambucil in 269 previously untreated patients ≥ 65 years of age (median age, 73 years) with CLL or SLL.[8] The authors reported major hemorrhage (≥ grade 3 or central nervous system hemorrhage of any grade) in 6 patients (4%) in the ibrutinib group. Three of the 6 patients subsequently discontinued ibrutinib; the authors also reported that 3 of the 6 patients were receiving concomitant low-molecular-weight heparin, aspirin, or vitamin E at the time of the event. The authors did not specify whether these were the same 3 patients who discontinued ibrutinib during this period. Of these 6 patients, the authors reported 1 with grade 4 intraparenchymal hemorrhage from transformation of ischemic stroke and 1 with grade 3 post-traumatic subdural hematoma. AF (ranging from grade 2 to 3) occurred in 8 patients (6%) receiving ibrutinib. Two of these patients discontinued ibrutinib. Seven of the 8 patients had a medical history significant for hypertension, coronary artery disease, or myocardial ischemia.
In 2015, Chanan-Khan and colleagues conducted a double-blind, placebo-controlled phase III trial assessing the safety and efficacy of adding ibrutinib (420 mg) to bendamustine plus rituximab (BR) vs placebo added to BR in 578 patients with relapsed or refractory CLL or SLL.[9] Patients were excluded from the trial if they had a history of stroke, intracranial hemorrhage, or clinically significant cardiovascular disease within the 6 months prior to randomization. Patients were also excluded if they required concomitant anticoagulation with warfarin or other vitamin K antagonists or strong CYP3A4/A5 inhibitors. Authors reported any-grade bleeding events in 89 patients (31%) in the ibrutinib group vs 42 patients (15%) in the placebo group. The authors reported major hemorrhage in 11 patients (4%). Six of the 11 patients were receiving concomitant anticoagulant or antiplatelet treatment. Major hemorrhage events required ibrutinib discontinuation in 2 of these 11 patients. Twenty-one patients (7%) in the ibrutinib group experienced AF (grade 1/2) vs 7 patients (2%) in the placebo group. Of note, 25 patients in the ibrutinib group had a history of AF or flutter; 7 of these patients developed AF or flutter during the study period. The authors reported that most patients with comorbid cardiac disorders at randomization did not develop AF or flutter. Of the 289 patients in the ibrutinib group, 4 (1%) discontinued ibrutinib therapy upon development of AF. Seven patients in the ibrutinib group had treatment withheld due to AF or flutter. These events resolved with no further AF episodes during the study period.
In 2016, Gustine and colleagues conducted a follow-up study characterizing IRAF in a cohort of 112 WM patients receiving ibrutinib therapy.[12] This study was initiated in response to the incidence of AF observed in the study conducted by Treon and colleagues in 2015 in a similar patient population.[7] This report did not address bleeding adverse events caused by ibrutinib. After a median follow-up time of 11.8 months with ibrutinib therapy, 12 patients (10.7%) were diagnosed with AF. Six of these 12 patients had a prior history of AF. Following AF diagnosis, 1 patient was started on warfarin and 1 patient was started on rivaroxaban. Of the 12 AF patients, 4 were managed with beta-blockers and 3 underwent cardioversion. Ibrutinib was held for 12 days in 5 of the 12 patients; all 5 patients resumed therapy after the 12-day period. Five of the 12 AF patients had a dose reduction of ibrutinib to 280 mg per day following the AF event. The authors note that despite an increased incidence of IRAF, the proven efficacy and safety of ibrutinib supports its use in patients with WM.
Applying the CHA2DS2-VASc and HAS-BLED Scoring Methods
Conventional management of AF requires a concomitant assessment of stroke and bleeding risk to select appropriate antithrombotic therapy. The CHA2DS2-VASc scoring system (Table 2) is used in the American College of Cardiology/American Heart Association (AHA)/Heart Rhythm Society guidelines to stratify patients into respective stroke risk categories, with corresponding suggested antithrombotic therapy (Tables 3, 4).[15,16] Likewise, the HAS-BLED score (Table 5) is useful for identifying and addressing modifiable bleeding risk factors associated with antithrombotic therapy (Table 6).[17,18] HAS-BLED has not been validated for use in practice.[19] Although these scoring systems are not validated in IRAF, balancing HAS-BLED along with CHA2DS2-VASc could help to optimize antithrombotic therapy in patients with IRAF.[17] Ultimately, antithrombotic therapy must be guided by discussions between the care team and the patient about preferences, risk of stroke and bleeding, and anticipated side effects. In addition, the patient must be aware that ibrutinib may increase the bleeding risk with anticoagulants, and that vigilant monitoring is warranted.[1] Because evidence has yet to emerge related to IRAF and subsequent thrombotic stroke, it may be prudent to offer rate or rhythm control alone, given the already elevated bleeding risk with the use of ibrutinib.
In addition to antithrombotic therapy for patients with AF, the AHA guidelines recommend ventricular rate control with a beta-blocker or a nondihydropyridine calcium channel blocker.[16] Heart rate and rhythm that do not normalize warrant rhythm control therapy, atrioventricular nodal ablation, or permanent ventricular pacing. Careful selection of rate- or rhythm-controlling medications is important. For example, verapamil and diltiazem are inhibitors of CYP3A4, a primary site for ibrutinib metabolism, and may increase ibrutinib serum concentration up to 900%.[1] Alternatively, ibrutinib may increase serum amiodarone drug concentrations through inhibition of p-glycoprotein, a ubiquitous cellular transport protein, leading to hypotension and a potential increased fall risk.[1]
For patients with IRAF, we propose calculating CHA2DS2-VASc and HAS-BLED scores to help estimate potential risks vs benefits of antithrombotic therapy. We recommend routine consultation with a cardiology specialist to determine the most appropriate intervention for AF (cardioversion, ablation, rate/rhythm control) to manage stroke risk.[19] However, because cardiologists may not be aware of bleeding risks associated with ibrutinib, we have proposed a treatment algorithm to help minimize drug-drug interactions that could inadvertently occur when initiating antiarrhythmic or rate control therapy for patients with IRAF (See Figure).
Clinical Scenario #1
A 70-year-old man with relapsed CLL was started on ibrutinib, at 420 mg once daily at bedtime, 6 months ago secondary to symptomatic splenomegaly. He has a history of hypertension but has never had a stroke. He presents with new onset of shortness of breath and palpitations. Heart rate is 152 beats/min and blood pressure is 88/52 mm Hg. Electrocardiogram is significant for AF.
Application of algorithm:
Is the patient stable?-No.
Proceed to rate/rhythm control. Diltiazem, verapamil, and amiodarone should be avoided because of potential drug interactions.
The patient is referred to the cardiology team, which recommends and performs an ablation.
Calculate CHA2DS2-VASc score: age 65–74 = 1 point, hypertension = 1 point; total score = 2.
Calculate HAS-BLED score: age > 65 = 1 point, hypertension = 1 point, drug use (ibrutinib) = 1 point; total score = 3.
Bleeding risk outweighs risk of stroke. Final recommendation: recommend no anticoagulation. If risk of stroke is unacceptable to the patient, consider changing to alternative CLL therapy with lower risk of bleeding in order to allow initiatiation of anticoagulation therapy. If patient agrees to forgo anticoagulation, restart ibrutinib.
Clinical Scenario #2
A 75-year-old woman with relapsed MCL was started on ibrutinib, at 560 mg once daily, 4 months ago at the time of relapse. She has a complex medical history that includes hypertension, prior thrombotic stroke, peripheral artery disease (PAD), and diabetes. The patient presents to her oncologist with dyspnea on exertion and fatigue. Vital signs reveal a heart rate of 166 beats/min and blood pressure of 110/70 mm Hg. Electrocardiogram is significant for AF.
Application of algorithm:
Is the patient stable?-No.
Proceed to rate/rhythm control. Diltiazem, verapamil, and amiodarone should be avoided because of potential drug interactions. Metoprolol is started.
The patient’s heart rate is reduced to 82 beats/min.
Calculate CHA2DS2-VASc score: age 65–74 = 1 point; hypertension = 1 point; prior stroke = 2 points; PAD = 1 point; diabetes = 1 point; female = 1 point; total score = 7 (adjusted thrombotic stroke rate, 9.6%/yr).
Calculate HAS-BLED score: age > 65 = 1 point; hypertension = 1 point; prior stroke = 1 point; drug use (ibrutinib) = 1 point; total score = 4.
Risk of stroke may outweigh risk of bleeding. Final recommendation: Decision will need to be individualized, taking into account patient preferences; the feasibility of rate or rhythm control; the patient’s disease history; the availability of effective alternative treatments for lymphoma; and the feasibility, effectiveness, and toxicity of various anticoagulation agents.
Restart ibrutinib, since patients do not respond well to post-ibrutinib therapies for MCL.[20]
Do not offer anticoagulant. Continue metoprolol and monitor for tolerability and effectiveness.
Discussion
The management of IRAF is particularly challenging when attempting to balance the risk of thromboembolic stroke due to AF, and the ensuing hemorrhagic risk resulting from concomitant antithrombotic therapy. Current evidence suggests that hemorrhagic risk is greater than that of thrombosis, perhaps owing to an inherent antithrombotic effect of ibrutinib therapy. The heterogeneity in inclusion and exclusion criteria and use of concomitant medications make the interpretation of clinical trial data challenging. The under-reporting of concomitant medications used in clinical trials is a prime example of limited external validity. In addition, it is well recognized that patients may have numerous comorbidities that could limit the applicability of evidence from clinical trials to real world practice.
For patients receiving ibrutinib who develop AF, we suggest calculating CHA2DS2-VASc and HAS-BLED scores in order to provide them and their treating physicians with a rough estimate, as a starting point, of the risk of a thromboembolic complication due to AF and the increased risk of bleeding with the addition of anticoagulation. We recognize that the risk of bleeding provided by the HAS-BLED score does not fully quantify the added risk of bleeding due to ibrutinib therapy. Thus, the HAS-BLED estimate essentially provides a lower-bound estimate of a bleeding complication, and the actual risk of a bleeding complication in patients who continue treatment with ibrutinib is likely higher. Nonetheless, these scores allow identification of a proportion of patients for whom the risk of a thromboembolic event is purported to be lower than the risk of bleeding. In these patients, ibrutinib should be continued without the addition of anticoagulation.
Patients with IRAF whose risk of stroke outweighs the risk of bleeding from anticoagulation should have a detailed discussion with their oncologist and cardiologist regarding the utility of rhythm control, rate control, anticoagulation, and treatment options for their lymphoma or leukemia. Patients with limited cancer treatment options should prioritize continued treatment on ibrutinib, and AF should be managed such that their treatment with ibrutinib is not interrupted. For example, these patients could undergo chemical or direct cardioversion with a short course of anticoagulation, during which ibrutinib would be held. Patients who choose to be managed with rate/rhythm control should understand that there would be a potentially increased risk of stroke if IRAF were not adequately controlled. Patients who are anticipated to have multiple other options for treatment based upon their leukemia or lymphoma diagnosis, comorbidities, and treatment history may weigh the risks associated with IRAF against the risks of other antineoplastics.
Conclusion
Appropriate management of comorbidities and concomitant medications is essential to maintaining adherence to oral tyrosine kinase inhibitor therapy, regardless of disease state. IRAF is seen in 6% to 11% of patients receiving ibrutinib.[1,6] It is not known whether initiation of anticoagulation after the development of IRAF will decrease thrombotic stroke risk without increasing hemorrhagic stroke risk. For IRAF, we propose an algorithm to help guide drug choices, minimize the potential for drug-drug interactions, and involve and educate the patient in treatment planning. It is our belief that there must be a compelling reason to initiate anticoagulation for IRAF, as there have been no reported cases of thrombotic stroke due to IRAF. We place more emphasis on the importance of rate/rhythm control and continuation of ibrutinib therapy, and less on the need for anticoagulation. Clinical trial validation using this model is needed.
Financial Disclosure:Dr. Halwani has received research funding from AbbVie and Pharmacyclics. Dr. Sweetenham has received research funding from Pharmacyclics. The other authors have no significant financial interest or other relationship with the manufacturers of any products or providers of any service mentioned in this article.
References:
1. Pharmacyclics LLC. Imbruvica(R) [package insert]. Sunnyvale, CA; November 2013.
2. Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369:32-42.
3. Byrd JC, Brown JR, O’Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371:213-23.
4. Byrd JC, Furman RR, Coutre SE, et al. Three-year follow-up of treatment-naive and previously treated patients with CLL and SLL receiving single-agent ibrutinib. Blood. 2015;125:2497-506.
5. Wang ML, Blum KA, Martin P, et al. Long-term follow-up of MCL patients treated with single-agent ibrutinib: updated safety and efficacy results. Blood. 2015;126:739-45.
6. Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2013;369:507-16.
7. Treon SP, Tripsas CK, Meid K, et al. Ibrutinib in previously treated Waldenstrom’s macroglobulinemia. N Engl J Med. 2015;372:1430-40.
8. Burger JA, Tedeschi A, Barr PM, et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med. 2015;373:2425-37.
9. Chanan-Khan A, Cramer P, Demirkan F, et al. Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double-blind, phase 3 study. Lancet Oncol. 2016;17:200-11.
10. Levade M, David E, Garcia C, et al. Ibrutinib treatment affects collagen and von Willebrand factor-dependent platelet functions. Blood. 2014;124:3991-5.
11. McMullen JR, Boey EJ, Ooi JY, et al. Ibrutinib increases the risk of atrial fibrillation, potentially through inhibition of cardiac PI3K-Akt signaling. Blood. 2014;124:3829-30.
12. Gustine JN, Meid K, Dubeau TE, et al. Atrial fibrillation associated with ibrutinib in Waldenstrom’s macroglobulinemia. Am J Hematol. 2016;91:E312-E313.
13. O’Brien S, Furman RR, Coutre SE, et al. Ibrutinib as initial therapy for elderly patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: an open-label, multicentre, phase 1b/2 trial. Lancet Oncol. 2014;15:48-58.
14. Kamel S, Horton L, Ysebaert L, et al. Ibrutinib inhibits collagen-mediated but not ADP-mediated platelet aggregation. Leukemia. 2015;29:783-7.
15. Mason PK, Lake DE, DiMarco JP, et al. Impact of the CHA2DS2-VASc score on anticoagulation recommendations for atrial fibrillation. Am J Med. 2012;125:603.e1-e6.
16. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1-e76.
17. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol. 2011;57:173-80.
18. Friberg L, Rosenqvist M, Lip GY. Net clinical benefit of warfarin in patients with atrial fibrillation: a report from the Swedish atrial fibrillation cohort study. Circulation. 2012;125:2298-307.
19. Loewen P, Dahri K. Risk of bleeding with oral anticoagulants: an updated systematic review and performance analysis of clinical prediction rules. Ann Hematol. 2011;90:1191-200.
20. Martin P, Maddocks K, Leonard JP, et al. Postibrutinib outcomes in patients with mantle cell lymphoma. Blood. 2016;127:1559-63.
21. Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138:1093-100.
22. Camm AJ, Lip GY, De Caterina R, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012;33:2719-47.













