LHRH Analog Bone Loss Recovers 1 Year After Treatment
SAN FRANCISCO-While bone mineral density decreases with ovarian ablation via the leutinizing hormone releasing hormone (LHRH) analog goserelin (Zoladex), the loss is partly recovered within a year after 2 years of treatment. Also, the loss may be minimized by the addition of tamoxifen (Nolvadex), according to an analysis of ZIPP (Zoladex in Premenopausal Patients) trial data presented at the 37th Annual Meeting of the American Society of Clinical Oncology (ASCO abstract 96).
SAN FRANCISCOWhile bone mineral density decreases with ovarian ablation via the leutinizing hormone releasing hormone (LHRH) analog goserelin (Zoladex), the loss is partly recovered within a year after 2 years of treatment. Also, the loss may be minimized by the addition of tamoxifen (Nolvadex), according to an analysis of ZIPP (Zoladex in Premenopausal Patients) trial data presented at the 37th Annual Meeting of the American Society of Clinical Oncology (ASCO abstract 96).
Ovarian Ablation
Ovarian ablation improves survival for premenopausal women with early breast cancer, said A. Sverrisdóttir, MD, Huddinge University Hospital, Stockholm, Sweden. The benefits of treatment with LHRH analogs have been comparable to the benefits of chemotherapy. Concerns remain, however, about inducing a premature menopause because of the known increased risk of bone mineral density loss with early menopause.
While it is known that tamoxifen has estrogen agonist effects, the potential adverse effects of LHRH analog treatment on bone are unknown, Dr. Sverrisdóttir said. Furthermore, the net effect of the combination of ovarian ablation and tamoxifen in premenopausal women is unknown.
In the ZIPP trial results presented at ASCO 2000, recurrence-free survival benefits for adjuvant therapy with goserelin were highly significant (P = .001) in premenopausal women with node-negative breast cancer who did not receive adjuvant chemotherapy.
Bone Mineral Density Data
For the current analysis, bone mineral density data from 73 Stockholm participants in the trial were evaluated. The patients received no adjuvant therapy (n = 22), tamoxifen (40 mg/d for 2 years, n = 19), goserelin alone (3.6 mg every 28 days for 2 years, n = 17), or tamoxifen plus goserelin (n = 15).


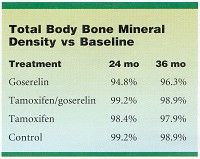
After 2 years of treatment, total body bone mineral content fell significantly in the goserelin group, compared with baseline (see Table . A year after the cessation of adjuvant therapy (at 36-months’ follow-up), however, total body bone mineral content increased significantly (+1.5%) in the goserelin group (see Table), while continuing to decrease in the others.
Dr. Sverrisdóttir summarized: "There was significant loss of bone with Zoladex. Tamoxifen alone had no statistically significant effect on total body bone mineral content, compared to untreated controls. However, tamoxifen appears to compensate for the demineralizing effect of Zoladex, and there was a significant regain of bone mineral density after cessation of Zoladex treatment."
She noted that future research needs to determine the effects of goserelin beyond 2 years of treatment, any age-related effects of goserelin or tamoxifen, and fracture risks related to changes in bone mineral density.














