(P149) Collimator Design and Optimization for an Ir-192 Based Small-Animal Irradiator
Small-animal irradiation is a critical part of translational studies in radiation oncology. The ability to deliver a small, highly focused radiation field allows for evaluation of radiation effects, as well as quantification of acute and late toxicities, in an assortment of tissues.


P149: Figure
Zachary C. Wilson, MD, Michael P. Grams, PhD, Kenneth W. Merrell, MD, MS, Terence S. Sio, MD, MS, Bradley J. Stish, MD, MS, Martha Hosotani, PhD, Katrina K. Bakken, Benjamin Mou, MD, FRCPC, Jann N. Sarkaria, MD; Mayo Clinic
Background: Small-animal irradiation is a critical part of translational studies in radiation oncology. The ability to deliver a small, highly focused radiation field allows for evaluation of radiation effects, as well as quantification of acute and late toxicities, in an assortment of tissues. We evaluated a variety of dense metals and alloys to sustain a radiobiologically meaningful dose rate (> 2 Gy/min) using Ir-192 and shield tissue outside of the primary field.
Materials and Methods: Using a 10-Ci Ir-192 source, we evaluated dose rate and effective shielding of variable-thickness lead and tungsten alloy. With theoretical half-value layers (HVLs) of 5 mm for lead and 3.3 mm for tungsten, we assessed in-field dose rates and doses at specific distances from the block edge using Gafchromic dosimetric film. Collimator dimensions were based on biometric measurements of mature athymic nude mice.
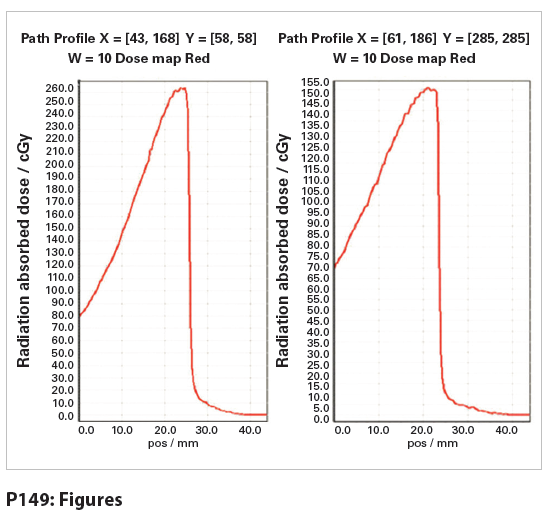
Results: Collimator dimensions were based on athymic nude mice hemibrain dimensions and measured 12 mm × 10 mm × 19 mm (length × width × depth) for the lead collimator. Tungsten collimator dimensions were 12 mm × 10 mm × 13.2 mm. Empirically measured density of the lead collimator was 10.92 g/cc and 19.0 g/cc for the tungsten collimator (tungsten/nickel alloy). Depth of the collimator was 4 theoretical HVLs for both lead and tungsten. Dose rates were 0.931 cGy/hr/mCi and 1.56 cGy/hr/mCi for lead and tungsten, respectively. The penumbra and dose profiles for each of the collimators are described, with the dose falling from a maximal dose rate of 260 cGy/min to 26 cGy over a span of 1.2 mm for the tungsten unit and from 155 cGy/min to 15 cGy/min over 1.3 mm for the lead unit.
Conclusions: Using a collimator of high-density tungsten alloy, we were able to deliver radiation at a radiobiologically meaningful dose rate to a small field. The tissue beyond the block edge was well shielded, with < 10% maximal dose received at ~1.5 mm from the collimator’s medial edge, based on Gafchromic dosimetric analysis. Due to the advantage of increased dose rate with the tungsten unit, this collimator design was implemented for a newly developed small-animal irradiator.









Targeted Therapy First Strategy Reduces Need for Chemotherapy in Newly Diagnosed LBCL
December 7th 2025Lenalidomide, tafasitamab, rituximab, and acalabrutinib alone may allow 57% of patients with newly diagnosed LBCL to receive less than the standard number of chemotherapy cycles without compromising curative potential.






