Peripheral T-cell Lymphomas: Their Time Has Come
Our ability to treat patients with B-cell lymphomas has improved dramatically over the past few decades. Today the majority of patients with diffuse large B-cell lymphoma are cured, the survival of patients with low-grade follicular lymphoma is improving (ie, some estimates have the average survival more than doubling), most patients with Hodgkin lymphoma (also a B-cell lymphoma) are cured, most patients with Burkitt lymphoma are cured, and our ability to diagnose and treat patients with the various marginal zone lymphomas has improved considerably.
Our ability to treat patients with B-cell lymphomas has improved dramatically over the past few decades. Today the majority of patients with diffuse large B-cell lymphoma are cured, the survival of patients with low-grade follicular lymphoma is improving (ie, some estimates have the average survival more than doubling), most patients with Hodgkin lymphoma (also a B-cell lymphoma) are cured, most patients with Burkitt lymphoma are cured, and our ability to diagnose and treat patients with the various marginal zone lymphomas has improved considerably. Among B-cell lymphomas, only mantle cell lymphoma has been slow to respond to our treatments. However, mantle cell lymphoma has only been recognized since the 1990s, and a variety of new drugs shown to be active in that disorder hold promise for future advances.
TABLE 1


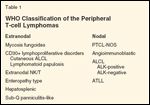
WHO Classification of the Peripheral T-cell Lymphomas
Unfortunately, the same cannot be said of the peripheral T-cell lymphomas. Until recently, these disorders were poorly characterized. Fortunately, the Revised European-American Lymphoma (REAL) classification, and its successor-the World Health Organization (WHO) classification-have dramatically improved our ability to classify these conditions into clinically relevant subgroups (Table 1). Pathologists are able to make the diagnosis, although still not as reproducibly as with B-cell lymphomas.
Most of the peripheral T-cell lymphomas are aggressive diseases, but mycosis fungoides and the CD30-positive cutaneous lymphoproliferative disorders are typically chronic illnesses with a prolonged natural history. Although the concept of CD30-positive cutaneous lymphoproliferative disorders is relatively recent, our understanding of these diseases is rapidly improving. Mycosis fungoides in advanced stages presents a very characteristic clinical syndrome. In the past decade, a number of new drugs have been approved for use in mycosis fungoides and offer the promise of improvement in our ability to benefit these patients.
Largely Ignored in Research
The aggressive peripheral T-cell lymphomas have been largely ignored in therapeutic research. They represent less than 10% of patients with lymphoma seen in the United States, and in the past have been included in clinical trials along with the much more common aggressive B-cell lymphomas. Since the treatment that most benefited patients with diffuse large B-cell lymphoma was the "winner" in these studies, it is perhaps not surprising that our ability to treat patients with aggressive peripheral T-cell lymphoma has not improved substantially. We have been treating patients with aggressive peripheral T-cell lymphoma as if they had a rare form of diffuse large B-cell lymphoma.
In fact, at the time this manuscript was written, there were no drugs specifically approved for the treatment of patients with aggressive peripheral T-cell lymphoma, although in the fall of 2009, pralatrexate (Folotyn) was approved by the US Food and Drug Administration. Of the aggressive peripheral T-cell lymphomas, only ALK-positive anaplastic large-cell lymphoma presenting in younger patients responds well to anthracycline-containing combination chemotherapy regimens. Better treatment for the other aggressive peripheral T-cell lymphomas is desperately needed. However, these represent a wide variety of clinical/pathologic syndromes, and it is unlikely that the same treatment will benefit all patients equally.
Biologically Diverse Subgroups
The most common aggressive peripheral T-cell lymphomas are usually nodal in origin. Angioimmunoblastic T-cell lymphoma has a relatively characteristic clinical picture, with widespread lymphadenopathy, system symptoms, and characteristic laboratory abnormalities. This appears to be a tumor of follicular helper T cells, and these patients sometimes develop Epstein-Barr virus (EBV)-driven diffuse large B-cell lymphoma. Adult T-cell lymphoma/leukemia is related to infection by human T-cell lymphotropic virus (HTLV)-1 and is geographically restricted in its occurrence. The largest group of aggressive peripheral T-cell lymphomas, peripheral T-cell lymphoma–not otherwise specified, often has the same clinical presentation as B-cell aggressive lymphoma, but a T-cell lymphoma is found on biopsy. It is becoming increasingly apparent that this is not a biologically uniform subgroup.
The only common aggressive extranodal peripheral T-cell lymphomas are the extranodal NK/T-cell tumors that typically present with involvement of the nasal sinuses and are highly EBV-associated. However, this type of peripheral T-cell lymphoma can present involving other organs. The rare extranodal aggressive peripheral T-cell lymphomas include the enteropathy type (ie, frequently associated with celiac disease), hepatosplenic lymphoma (which frequently causes diagnostic dilemmas and typically presents as a systemic illness in young males), and subcutaneous panniculitis-like T-cell lymphoma (which has a more indolent course and is often associated with a delayed diagnosis because the disease is confused with panniculitis).
A New Focus
With this issue, ONCOLOGY is initiating a special series on the peripheral T-cell lymphomas, beginning with Dr. Marshall E. Kadin's "Current Management of Primary Cutaneous CD30+ T-cell Lymphoproliferative Disorders." Subsequent installments will deal with mycosis fungoides, adult T-cell leukemia/lymphoma, peripheral T-cell lymphoma–unspecified, anaplastic large-cell lymphoma, angioimmunoblastic T-cell lymphoma, nasal NK T-cell lymphoma, and the rare T-cell lymphomas with extranodal presentations.
It is certainly time to focus on these lymphomas. There is no reason to doubt that better understanding of their biology and making them a priority in therapeutic research will improve survival. The peripheral T-cell lymphomas have largely represented a therapeutic wasteland. It is high time that this changes.
Financial Disclosure: Dr. Armitage is a consultant for Allos Therapeutics and Eisai.














