Erdafitinib in the Treatment of Metastatic Urothelial Carcinoma
Francisco Castro-Alonso, MD, and colleagues describe the effects of the use of erdafitinib in a patient with metastatic urothelial bladder cancer.



The Case
A Hispanic man, aged 42 years, was diagnosed with stage IV metastatic urothelial bladder cancer (MUBC) with nonregional lymphadenopathies and lung, bone, and skin involvement. He received first-line treatment with gemcitabine and cisplatin for 6 cycles, achieving a partial response (PR). Next, he received immunotherapy maintenance with avelumab for 4 months until disease progression. A next-generation sequencing test of paraffin-embedded tumor tissue identified a fibroblast growth factor receptor 3 (FGFR3) S249C missense mutation.
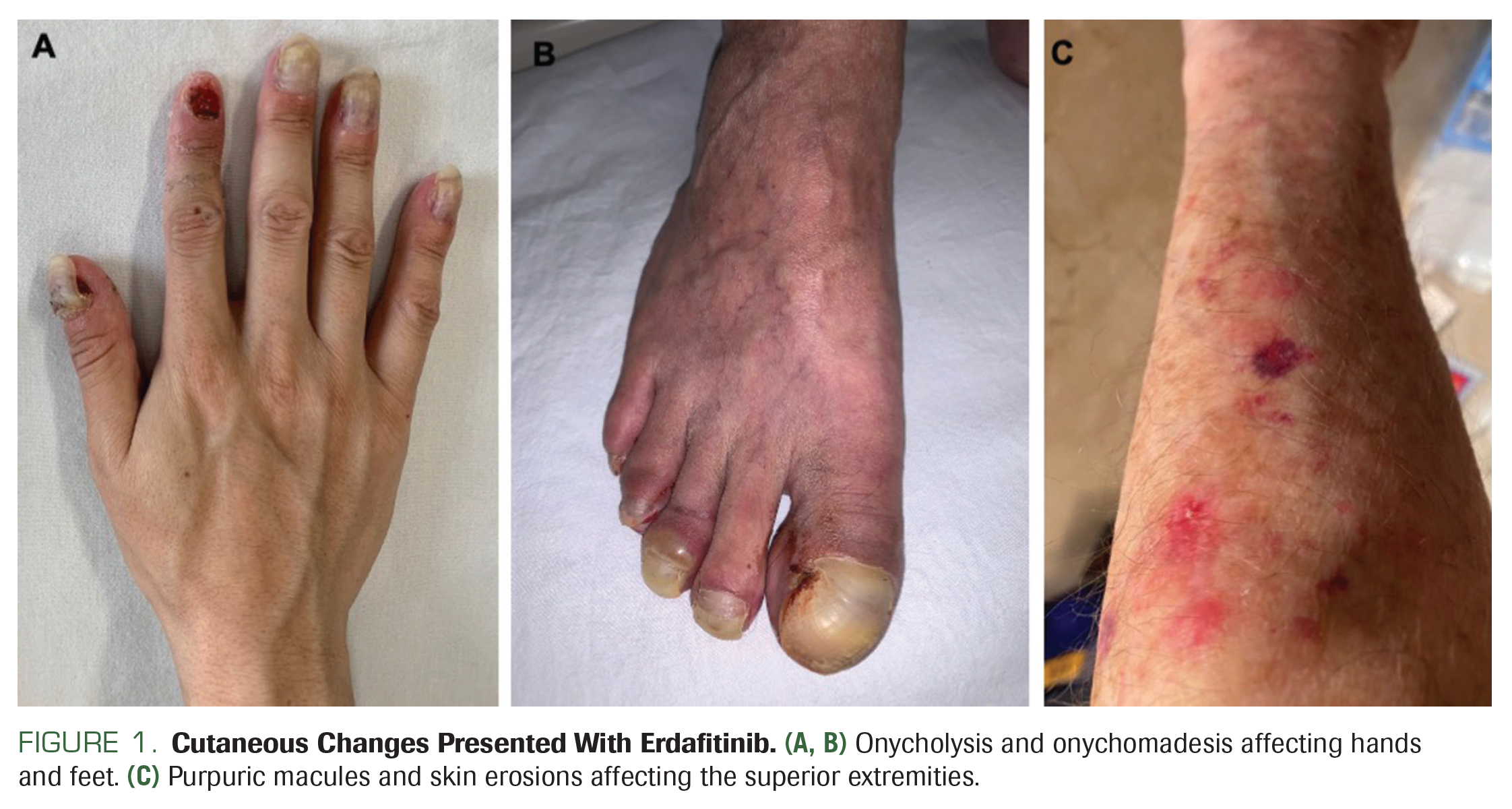
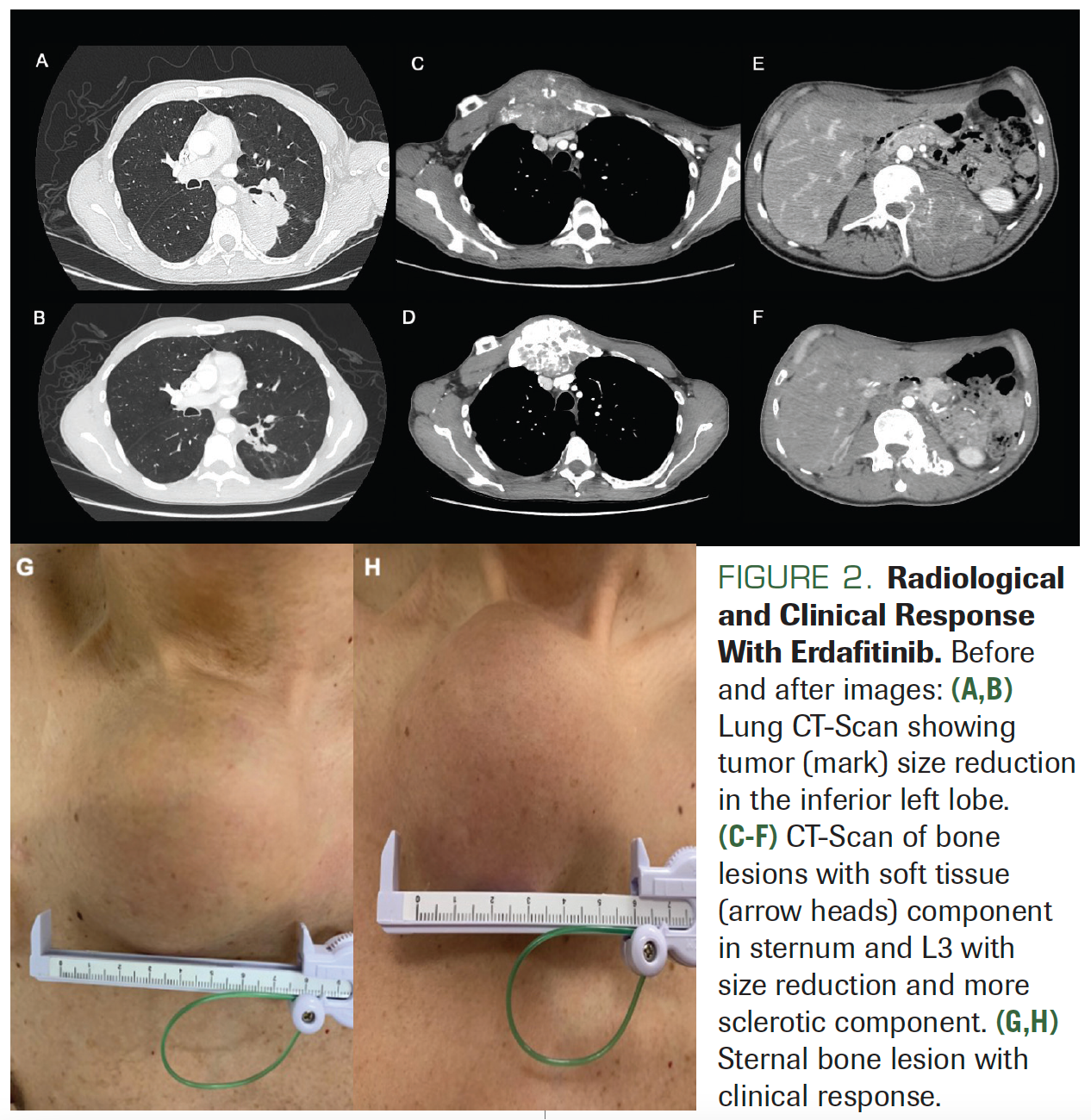
The patient was started on erdafitinib 8 mg daily, and while he was on this dosage, he presented with grade 2 hyperphosphatemia of 8 mg/dL. Erdafitinib treatment was temporarily withheld until his phosphorus level reached less than 5.5 mg/dL, accomplished with dietary phosphate restriction to 600 to 800 mg/ day; then, erdafitinib was restarted at the same dose. Thereafter, he experienced onycholysis, onychomadesis, Beau lines, and paronychia, with purpuric skin lesions and erosions (Figures 1A-1C). Grade 2 nail loss with superinfection was diagnosed and erdafitinib treatment was delayed for 14 days with weekly reassessment. He received oral trimethoprim/sulfamethoxazole for 2 weeks with improvement of symptoms to grade 1. Afterward, he restarted erdafitinib with a dose reduction to 6 mg daily, resulting in better tolerance. The patient achieved clinical response with reduction of metastatic bone lesions, and a CT scan at 10 weeks after he began erdafitinib revealed a PR according to RECIST criteria (Figures 2A-2H).
Oncology (Williston Park). 2023;37(6):256-261.
DOI: 10.46883/2023.25920998




Which of the following statements about erdafitinib is incorrect?
A. Either FGFR3 mutations or FGFR2/3 fusions are required for its therapeutic use.
B. Phosphorus serum levels are recommended to guide dose titration.
C. Hyperphosphatemia is the most common adverse event (AE) associated with erdafitinib use.
D. FDA approval was based on a phase 2 trial for patients progressing after platinum therapy with or without immunotherapy.
E. Lower phosphorus levels are associated with better outcomes.
Platinum-based chemotherapy is the standard first-line treatment for patients with MUBC, with either cisplatin or carboplatin combinations.1-4 In patients whose disease does not progress on chemotherapy, maintenance with avelumab is indicated.4 This evidence comes from the JAVELIN-100 Bladder study (NCT02603432), a phase 3 randomized clinical trial that showed an overall survival (OS) improvement of 7.1 months (median OS, 21.4 vs 14.3 months; HR, 0.69) and a progression-free survival (PFS) benefit of 1.7 months (median PFS, 3.7 vs 2.0 months; HR, 0.62) when comparing avelumab with best supportive care.5
Despite these improvements in survival with avelumab, most patients will inevitably progress after chemotherapy and immunotherapy, warranting subsequent treatment options. In this scenario, treatments involving antibody-drug conjugates (ADCs) and tyrosine kinase inhibitors (TKIs) have shown promising results.6-8 Among the ADCs, enfortumab vedotin (EV), an antinectin-4 antibody coupled to an antimicrotubule payload, has the strongest evidence, and is considered the standard of care in patients who progress after chemotherapy and immunotherapy. This is based on a phase 3 trial in which patients were randomly assigned to receive EV or investigator-chosen chemotherapy (docetaxel, paclitaxel, or vinflunine). Patients who received EV had significantly better OS (12.8 vs 8.9 months; HR, 0.7), PFS (5.5 vs 3.7 months; HR, 0.62), and overall response rate (ORR; 40.6% vs 17.9%).6 Additionally, another ADC, sacituzumab govitecan (SG)—a Trop-2 antibody associated with a topoisomerase I inhibitor—was approved by the FDA in 2021 based on the results of cohort 1 of the TROPHY-U-01 study (NCT03547973). This phase 2 trial evaluated SG in patients who had already received platinum-based chemotherapy and a checkpoint inhibitor. The primary end point, ORR, was 27.7%; the mean duration of response was 7.2 months and the median PFS and OS were 5.4 and 10.9 months, respectively.7
Targeted therapies against driver mutations have been used in cancer treatment for more than 4 decades;8 in MUBC, inhibition of FGFR alterations is of the utmost importance.8,9 FGFR comprises a family of 4 transmembrane protein kinases that are normally involved in embryogenesis and tissue proliferation10 and FGFR5 exhibits an absence of intracellular tyrosine kinase domain, resulting in the lack of receptor tyrosine kinase activity.22 Cancer-cell alterations in this pathway cause constitutive activation of the receptor, resulting in cellular proliferation, migration, and survival.10,11 Across different cancer types, urothelial carcinoma harbors the highest frequency of FGFR alterations (15%-20%),8,10,11 with FGFR3 point mutations being the most common, followed by FGFR3 fusions.12
Efforts to inhibit FGFR alterations in MUBC are not new. The first attempt to target this receptor was with dovitinib, a multikinase TKI with FGFR activity. In 2013, results of a phase 2 trial (NCT00790426) reported that the drug had limited activity.13 Newer, more specific FGFR inhibitors have since been developed, including the TKIs pemigatinib, rogaratinib, infigratinib, futibatinib, derazantinib, and AZD454, as well as the monoclonal antibody vofatamab.9,14,15 Other than erdafitinib, all of these drugs are currently used only in clinical trials.
Erdafitinib’s clinical benefit was first demonstrated in a phase 1 trial, from which 2 dosing strategies were recommended for further research: a continuous 9-mg daily dose, and an intermittent 10 mg/day schedule, alternating 7 days on and 7 days off.16
Erdafitinib was further studied in BLC2001, a phase 2 clinical trial that included 99 patients with unresectable, locally advanced or MUBC. All patients had either an FGFR3 mutation or fusions of FGFR2/3, and all had progressed during or after 1 or more prior lines of chemotherapy and anti–PD-1 or anti–PD-L1 blockade. The primary end point was ORR. BLC2001 was initially designed as a 2-arm trial, with each arm studying the continuous and intermittent regimens previously recommended by the phase 1 trial. After a protocol amendment, however, a continuous daily 8-mg dose was selected, with the possibility of up-titration according to serum phosphate levels. After a median follow-up of 11 months, the ORR was 40%, with 3% complete responses and 37% PRs. The mean PFS and OS were 5.5 and 13.8 months, respectively.17 Based on these unprecedented results, erdafitinib was authorized by the FDA in 2019 for the treatment of MUBC. Therefore, answers A and D are correct.


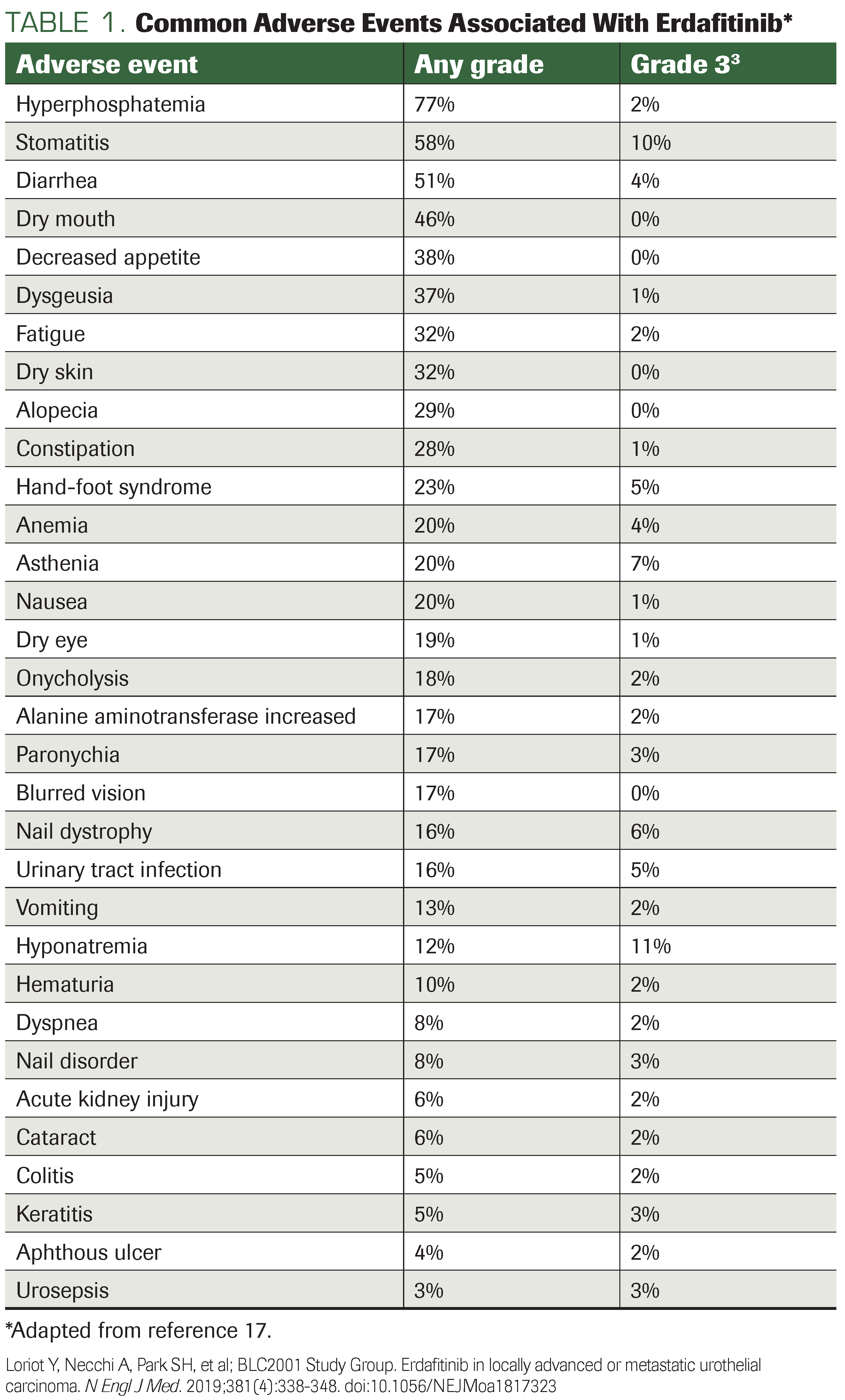
In BLC2001, 100% of patients reported having AEs of any cause; hyperphosphatemia was the most common (77%), followed by stomatitis (58%), diarrhea (51%), and xerostomia (46%). Grade 3, 4, and 5 AEs of any cause were reported in 67% of patients; hyponatremia and stomatitis were the most frequent (11% and 10%, respectively). The Table presents a more comprehensive list of AEs.17 Real-world data show a similar profile. Of 12 patients in a Brazilian series who were receiving erdafitinib as a second-line treatment, 83% reported any-grade AEs, and 42% reported grade 3/4 AEs; again, any-grade hyperphosphatemia was the most common (33%).18 Thus, answer C is correct.
The etiology underlying the development of hyperphosphatemia in a substantial proportion of patients receiving erdafitinib is related to the wide range of functions of FGFR, a tyrosine kinase expressed on the cell membrane involved in cell proliferation, survival, migration, and differentiation.19 Physiologically, in the proximal renal tubule FGFR1 is activated by its interaction with its ligand in the presence of the Klotho transmembrane protein; this inhibits the reabsorption of phosphate by NaPi-2a, a sodium-phosphate cotransporter, and blocks the conversion of 25-hydroxyvitamin D to 1,25-hydroxyvitamin D. This limits the absorption of phosphate by the small intestine.20 Hyperphosphatemia is so common that it is considered to be a marker of FGFR inhibition, and it is used for erdafitinib dose titration, with a target serum level of 5.5 to 7.0 mg/dL.17 There is evidence that higher efficacy of erdafitinib correlates with high serum phosphorus level. In the pivotal phase 2 trial, when comparing patients with phosphorus levels greater than vs less than 5.5 mg/ dL, the ORR was 42.7% vs 34.8%, respectively, median PFS was 5.6 vs 3.8 months (HR, 0.68), and median OS was not reached vs 6.7 months (HR, 0.35).21 Therefore, answer B is correct.
Because higher phosphorus levels, rather than lower levels, are associated with better outcomes, answer E is incorrect and thus is the question’s proper response.
Skin toxicity associated with erdafitinib, although it occurs less frequently than hyperphosphatemia, can represent more of a challenge. In the pivotal phase 2 trial evaluating erdafitinib for MUBC, 16% of patients underwent dose reductions due to skin toxicity.17 Management of skin AEs associated with TKI use is different than management of those caused by chemotherapy; supportive measures include emollients and, if those are not effective, topical steroids.22-24 Nail toxicity is particularly difficult to manage. The most common AEs reported in the BLC2001 trial were onycholysis (16%), nail dystrophy (16%), and paronychia (14%); of the 13 patients who suspended the treatment due to serious AEs, 2 did so due to nail AEs.17 Patients can try to prevent these events with lifestyle measures, which include avoiding prolonged contact with water, wearing loose-fitting socks and footwear, wearing gloves to avoid trauma, and refraining from biting or cutting nails too short. Nail hardeners are a further option. Oral antibiotics are indicated if secondary infection develops.22-24
Level A evidence regarding treatment sequencing in MUBC is pending; however, we have retrospective evidence. In a single-center retrospective cohort of 80 patients who received EV, 26 patients harbored FGFR3 alterations. Although 8 patients were exposed to erdafitinib before EV, only 1 patient received erdafitinib afterward. When compared with patients who were FGFR-negative, those who were FGFR-positive and had no prior exposure to erdafitinib had a significantly shorter median PFS and a trend to shorter median OS on EV: 2.5 vs 6.8 months (HR, 0.3; P < .01) and 4.9 vs 14.6 months (HR, 0.42; P > .05), respectively. In contrast, patients with FGFR-altered with prior erdafitinib exposure showed similar median PFS with EV compared with the entire cohort: 6.7 vs 5.2 months.25 Tumor response also seems to be hindered in the patients who have FGFR2/3 activating mutations. In a multicenter cohort of 40 patients exposed to EV without prior erdafitinib exposure, ORR differed widely from those who had an FGFR2/3 mutations compared with those who did not (29% vs 55%), without statistical significance (P = .4) but larger studies are necessary to confirm this data.26 Erdafitinib’s place in the treatment sequencing in MUBC will be further studied in the ongoing THOR phase 3 multicohort trial (NCT03390504). In cohort 1, patients with FGFR3 alterations with MUBC who previously received anti-PD-1/ PD-L1 treatment and no more than 2 previous lines of systemic treatment, will be randomized to receive erdafitinib or chemotherapy with either docetaxel or vinflunine; in cohort 2, patients with FGFR3 alterations with MUBC who progressed on chemotherapy will be randomly assigned to erdafitinib or pembrolizumab in the second-line setting.27
Combination strategies are also an active area of clinical research. Some authors consider FGFR-altered tumors to be less immunogenic than those without FGFR pathway aberrancies.28,29 Combinations of FGFR inhibitors with anti– PD-1/anti–PD-L1 agents have been studied in several phase 2 studies, including the NORSE (erdafitinib plus cetrelimab; NCT03473743), FORT-2 (rogaratinib plus atezolizumab; NCT03473756), FIERCE-22 (vofatamab plus pembrolizumab; NCT03123055) and FIGHT-205 (pemigatinib plus pembrolizumab; NCT04003610) trials. Erdafitinib has also been studied in combination with EV in a phase 1B trial (NCT04963153).15 Larger confirmatory trials are eagerly awaited, as these may change the way we treat MUBC.
Case Outcome
After a PFS of 5 months, the patient presented with clinical and radiological progression. At this point, because the patient did not have access to EV or SG, he was offered additional chemotherapy. He received 2 cycles of docetaxel, but he experienced progressive disease and further clinical deterioration. He then began receiving best supportive care and died within 1 month due to disease progression.
AUTHOR AFFILIATIONS:
Francisco Castro-Alonso, MD;1 Evelyn Beas-Lozano, MD;2 Yuly A. Remolina-Bonilla, MD;2 Thomas W. Flaig, MD;3 and Maria T. Bourlon, MD, MSc2
1Department of Internal Medicine, ISSSTE Hospital Regional Presidente Juarez, Oaxaca, Mexico
2Department of Hematology and Oncology, Instituto Nacional de Ciencias Médicas y Nutrición Salvador y Zubirán, Mexico City, Mexico
3Division of Medical Oncology, University of Colorado School of Medicine, Aurora, CO, United States.
CORRESPONDING AUTHOR:
Maria T. Bourlon, MD, MSc
Department of Hematology and Oncology
Instituto Nacional de Ciencias Médicas y Nutrición Salvador y Zubirán
15 Vasco de Quiroga Street
Section XVI, Tlalpan
Ciudad de Mexico 14000, Mexico
Email: maitebourlon@gmail.com
CONFLICT OF INTEREST:
Francisco Castro-Alonso MD: Janssen & Johnson, MSD, Merk, Roche.
Evelyn Beas-Lozano MD: None
Yuly A. Remolina-Bonilla MD: MSD, Pfizer
Thomas W. Flaig MD: Novartis, Bavarian Nordic, Dendreon, GTx, Janssen Oncology, Medivation, Sanofi, Pfizer, Bristol Myers Squibb, Roche/Genentech, Exelixis, Aragon Pharmaceuticals, Sotio, Tokai Pharmaceuticals, AstraZeneca/MedImmune, Lilly, Astellas Pharma, Agensys, Seagen Inc, La Roche-Posay, Merck
Maria T Bourlon MD MS: Janssen & Johnson, Merk, Pfizer, MSD, Gilead, Astellas Pharma, Bristol Myers Squibb.
FINANCIAL DISCLOSURES: None.
REFERENCES
- Sternberg CN, de Mulder PH, Schornagel JH, et al; European Organisation for Research and Treatment of Cancer Genitourinary Tract Cancer Cooperative Group. Randomized phase III trial of high-dose-intensity methotrexate, vinblastine, doxorubicin, and cisplatin (MVAC) chemotherapy and recombinant human granulocyte colony-stimulating factor versus classic MVAC in advanced urothelial tract tumors: European Organization for Research and Treatment of Cancer Protocol no. 30924. J Clin Oncol. 2001;19(10):2638-2646. doi:10.1200/JCO.2001.19.10.2638
- Kaufman D, Raghavan D, Carducci M, et al. Phase II trial of gemcitabine plus cisplatin in patients with metastatic urothelial cancer. J Clin Oncol. 2000;18(9):1921-1927. doi:10.1200/JCO.2000.18.9.1921
- von der Maase H, Sengelov L, Roberts JT, et al. Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. J Clin Oncol. 2005;23(21):4602-4608. doi:10.1200/JCO.2005.07.757
- NCCN. Clinical Practice Guidelines in Oncology. Bladder cancer, version 1.2022. Accessed March 2, 2022. https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf
- Powles T, Park SH, Voog E, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med. 2020;383(13):1218-1230. doi:10.1056/NEJMoa2002788
- Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab vedotin in previously treated advanced urothelial carcinoma. N Engl J Med. 2021;384(12):1125-1135. doi:10.1056/NEJMoa2035807
- Tagawa ST, Balar AV, Petrylak DP, et al. TROPHY-U-01: a phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol. 2021;39(22):2474-2485. doi:10.1200/JCO.20.03489
- Audisio M, Tucci M, Di Stefano RF, et al. New emerging targets in advanced urothelial carcinoma: is it the primetime for personalized medicine? Crit Rev Oncol Hematol. 2022;174:103682. doi:10.1016/j.critrevonc.2022.103682
- Zengin ZB, Chehrazi-Raffle A, Salgia NJ, et al. Targeted therapies: expanding the role of FGFR3 inhibition in urothelial carcinoma. Urol Oncol. 2022;40(2):25-36. doi:10.1016/j.urolonc.2021.10.003
- Weaver A, Bossaer JB. Fibroblast growth factor receptor (FGFR) inhibitors: a review of a novel therapeutic class. J Oncol Pharm Pract. 2021;27(3):702-710. doi:10.1177/1078155220983425
- Ertl IE, Shariat SF, Mostafaei H, Ilijazi D, Loriot Y. Fibroblast growth factor receptors across urothelial carcinoma landscape. Curr Opin Urol. 2020;30(4):557-565. doi:10.1097/MOU.0000000000000782
- Garje R, An J, Obeidat M, Kumar K, Yasin HA, Zakharia Y. Fibroblast growth factor receptor (FGFR) inhibitors in urothelial cancer. Oncologist. 2020;25(11):e1711-e1719. doi:10.1634/theoncologist.2020-0334
- Milowsky MI, Dittrich C, Duran Martinez I, et al. Final results of a multicenter, open-label phase II trial of dovitinib (TKI258) in patients with advanced urothelial carcinoma with either mutated or nonmutated FGFR3. J Clin Oncol. 2013;31(suppl 6):abstr 255. doi:10.1200/jco.2013.31.6_suppl.255
- Szklener K, Chmiel P, Michalski A, Mańdziuk S. New directions and challenges in targeted therapies of advanced bladder cancer: the role of FGFR inhibitors. Cancers (Basel). 2022;14(6):1416. doi:10.3390/cancers14061416
- Peng J, Sridhar S, Siefker-Radtke AO, Selvarajah S, Jiang DM. Targeting the FGFR pathway in urothelial carcinoma: the future is now. Curr Treat Options Oncol. 2022;23(9):1269-1287. doi:10.1007/s11864-022-01009-4
- Bahleda R, Italiano A, Hierro C, et al. Multicenter phase I study of erdafitinib (JNJ-42756493), oral pan-fibroblast growth factor receptor inhibitor, in patients with advanced or refractory solid tumors. Clin Cancer Res. 2019;25(16):4888-4897. doi:10.1158/1078-0432.CCR-18-3334
- Loriot Y, Necchi A, Park SH, et al; BLC2001 Study Group. Erdafitinib in locally advanced or metastatic urothelial carcinoma. N Engl J Med. 2019;381(4):338-348. doi:10.1056/NEJMoa1817323
- Monteiro FSM, Gonçalves E Silva A, de S Gomes AJP, et al. Erdafitinib treatment in Brazilian patients with metastatic urothelial carcinoma (mUC): real-world evidence from an Expanded Access Program. Ther Adv Med Oncol. 2021;13:17588359211015499. doi:10.1177/17588359211015499
- Chae YK, Ranganath K, Hammerman PS, et al. Inhibition of the fibroblast growth factor receptor (FGFR) pathway: the current landscape and barriers to clinical application. Oncotarget. 2017;8(9):16052-16074. doi:10.18632/oncotarget.14109
- Boyce AM, Lee AE, Roszko KL, Gafni RI. Hyperphosphatemic Tumoral Calcinosis: Pathogenesis, Clinical Presentation, and Challenges in Management. Front Endocrinol (Lausanne). 2020 May 8;11:293. doi: 10.3389/fendo.2020.00293.
- Tagawa S, Siefker-Radtke A, Dosne AG, et al. Hyperphosphatemia due to erdafitinib (a pan-FGFR Inhibitor) and anti-tumor activity among patients (pts) with advanced urothelial carcinoma (UC). Ann Oncol. 2019;30(suppl_5):V375. doi:10.1093/annonc/mdz249.031
- Kommalapati A, Tella SH, Borad M, Javle M, Mahipal A. FGFR inhibitors in oncology: insight on the management of toxicities in clinical practice. Cancers (Basel). 2021;13(12):2968. doi:10.3390/cancers13122968
- Lacouture ME, Sibaud V, Anadkat MJ, et al. Dermatologic adverse events associated with selective fibroblast growth factor receptor inhibitors: overview, prevention, and management guidelines. Oncologist. 2021;26(2):e316-e326. doi:10.1002/onco.13552
- Férez-Blando K, Castro-Alonso F, Domínguez-Cherit J, Bourlon MT. Hand-foot skin reaction secondary to sunitinib in a patient with metastatic clear cell renal cell carcinoma. Oncology (Williston Park). 2021;35(5):272-276. doi:10.46883/ONC.2021.3505.072
- Teo MY, Ratna N, Regazzi AM, et al. Enfortumab vedotin in FGFR3-mutated advanced urothelial carcinoma. J Clin Oncol. 2021;39(suppl 6):abstr 458. doi:10.1200/JCO.2021.39.6_suppl.458
- Adib E, Jain RK, Skelton WP, et al. Impact of FGFR2/3 activating genomic alterations on response to enfortumab vedotin in metastatic urothelial carcinoma (mUC). J Clin Oncol. 2021;39(suppl 6):abstr 472. doi:10.1200/JCO.2021.39.6_suppl.472
- A study of erdafitinib compared with vinflunine or docetaxel or pembrolizumab in participants with advanced urothelial cancer and selected fibroblast growth factor receptor (FGFR) gene aberrations (THOR). ClinicalTrials.gov. Updated July 14, 2022. Accessed January13,2023.https://clinicaltrials.gov/ct2/show/NCT03390504
- Sweis RF, Spranger S, Bao R, et al. Molecular drivers of the non-T-cell-inflamed tumor microenvironment in urothelial bladder cancer. Cancer Immunol Res. 2016;4(7):563-568. doi:10.1158/2326-6066.CIR-15-0274
- Wang L, Gong Y, Saci A, et al. Fibroblast growth factor receptor 3 alterations and response to PD-1/PD-L1 blockade in patients with metastatic urothelial cancer. Eur Urol. 2019;76(5):599-603. doi:10.1016/j.eururo.2019.06.025