Radiotherapy Not Needed in Older Lumpectomy Patients With Early Cancer
SAN FRANCISCO-Preliminary results of a randomized Intergroup trial (CALGB, RTOG, ECOG) strongly suggest that radiotherapy should not be added to tamoxifen (Nolvadex) in older women who have undergone lumpectomy for early-stage breast cancer, said Kevin S. Hughes, MD, Department of Surgical Oncology, Massachusetts General Hospital, Boston.
SAN FRANCISCOPreliminary results of a randomized Intergroup trial (CALGB, RTOG, ECOG) strongly suggest that radiotherapy should not be added to tamoxifen (Nolvadex) in older women who have undergone lumpectomy for early-stage breast cancer, said Kevin S. Hughes, MD, Department of Surgical Oncology, Massachusetts General Hospital, Boston.
Speaking at the 37th American Society of Clinical Oncology annual meeting (abstract 93), Dr. Hughes reported data comparing tamoxifen plus radiotherapy with tamoxifen alone in 647 women (636 eligible), age 70 and older, with estrogen-receptor (ER) positive tumors who had undergone lumpectomy.
"Radiation therapy may not have clinical benefit or an impact on survival in this population," Dr. Hughes stated. "In older patients, tumors tend to grow more slowly, and there is a lower risk of in-breast recurrence and a shorter time at risk. Data show that the standard of care should remain unchanged for these women at this period of follow-up."
Dr. Hughes reported that with a median follow-up of 28 months, the rate of locoregional failure was very low in both treatment groups and not significantly different.


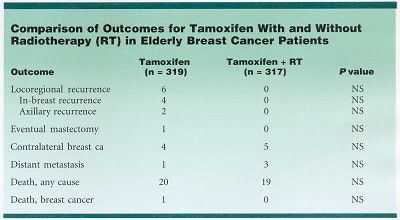
Of 317 patients receiving radiotherapy plus tamoxifen, none had a locoregional occurrence, compared with 6 of 319 patients on tamoxifen alone.
"The combination of tamoxifen plus radiotherapy may be superior for controlling locoregional breast cancer recurrences," Dr. Hughes said. "Longer follow-up is needed to fully assess whether this decrease is clinically important."
The rates of distant metastasis, eventual mastectomy, and contralateral breast cancer were similar in both arms.
There were no significant differences in overall, disease-free, or breast-cancer-specific survival between the treatment groups. Recurrence-free survival was 94% with tamoxifen and 100% with tamoxifen plus radiotherapy. Significantly, 6% of patients died on study, all but one from causes other than breast cancer.











 as a biosimilar to pertuzumab (Perjeta) in breast cancer, based on a review of various attributes, including safety and efficacy data.")




