43 Lobular Cancer Responsiveness to Chemotherapy Is Equivalent to That of Ductal Cancer With Similar Genomic Profiles: An NCDB Analysis
1University of Texas Medical Branch, Galveston, TX (roweiser@utmb.edu).
2University of Texas Medical Branch, Galveston, TX.
3The University of Texas MD Anderson Cancer Center, Houston, TX.
Background
Invasive lobular carcinoma (ILC) is traditionally considered less responsive to chemotherapy. While Oncotype recurrence score (RS) has been validated to identify high-risk patients who benefit from chemotherapy, some studies have questioned its relevance in patients with ILC. We sought to better characterize the potential use of RS in patients with ILC.
Materials and Methods:
The National Cancer Database (NCDB) was used to identify 3505 women with stage I to III, T1-T3, N1, hormone receptor–positive, HER2-negative ILC between 2010 and 2016, with an available RS. A similar cohort of 20,928 patients with invasive ductal carcinoma (IDC) was identified for comparison. Univariate analyses were used to identify variables correlating with chemotherapy use and 5-year survival. The Kaplan-Meier method was used to calculate 5-year survival. Subgroup analysis according to RS was performed.
Results
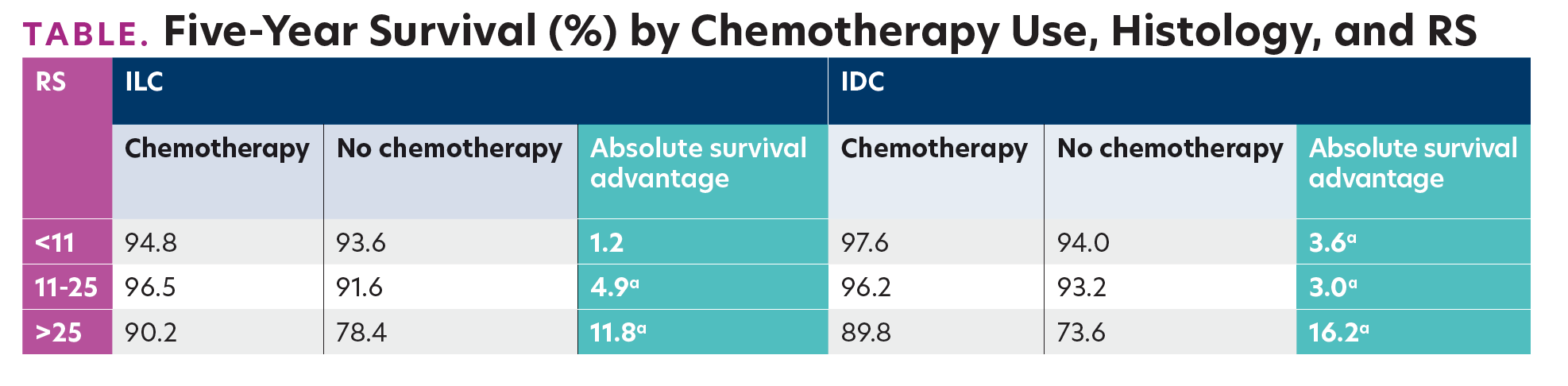
The mean age of ILC and IDC patients was 60.9 (±10.4) and 59.5 (±11.0) years, respectively. Patients with ILC had larger tumors, lower-grade disease, and a greater quantity of involved lymph nodes, and they received more mastectomies compared with patients with IDC. Fewer patients with ILC received chemotherapy compared with those with IDC (28.5% vs 34.9%; P <.0001). Patients with ILC had a lower mean (SD) RS (15.3 [±6.7] vs 17.1 [±10.1]; P <.0001), as well as a lower percentage of patients with high RS, defined as >25 (5.9% vs 14.7%; P <.0001). Among patients with high RS with ILC, 66.7% received chemotherapy compared with 79.4% of similar patients with IDC. A statistically significant absolute 5-year survival advantage was found in association with chemotherapy use in high-RS patients with ILC (11.8%), comparable with that in similar patients with IDC (16.2%). Intermediate-RS patients (RS, 12-25) with ILC and IDC demonstrated a more modest, but still statistically significant, survival advantage with chemotherapy: 4.9% and 3.0%, respectively (Table).

 by Chemotherapy Use, Histology, and RS")
TABLE. Five-Year Survival (%) by Chemotherapy Use, Histology, and RS
Conclusions
Patients with high-RS ILC are treated less often with chemotherapy compared with similar patients with IDC. Nevertheless, our data show an association between survival benefit and chemotherapy use in patients with high-RS ILC, and even intermediate-RS ILC. Such benefit should be taken into account when considering adjuvant chemotherapy in these patients.


Expert Commentary