Therapeutic Options Following Orchiectomy for Stage I Seminoma
Over the past 3 decades, the incidence rate of testicular seminoma has continually risen, and the majority of cases have been clinical stage I.[1] Nevertheless, the overall survival for all testicular cancers has improved significantly (P < .05) over the same period, from 83% to 96%.[2]
ABSTRACT: Stage I seminoma represents the paradigm of a curable malignancy, with survival of 100% an expected outcome no matter what treatment option is chosen. However, consensus has not been reached among urologists and oncologists regarding the optimal postoperative management in men with clinical stage I testicular seminoma. Currently, men are offered active surveillance, adjuvant radiation therapy, or single-agent chemotherapy. Active surveillance is associated with an 80% chance of no relapse, with all such events salvageable. Radiotherapy has an almost universal cure rate but has the potential for long-term toxicities and an overtreatment rate of about 80%. Chemotherapy efficacy and toxicity data are still immature. Recent guidelines recognize that the options of surveillance, chemotherapy, and radiotherapy are appropriate in the treatment of patients with clinical stage I seminoma. We believe active surveillance to be the best option, then radiotherapy (considering the efficacy and safety data), with single-agent chemotherapy emerging as a possible alternative.


Over the past 3 decades, the incidence rate of testicular seminoma has continually risen, and the majority of cases have been clinical stage I.[1] Nevertheless, the overall survival for all testicular cancers has improved significantly (P < .05) over the same period, from 83% to 96%.[2]
Seminomas generally have a lower stage at diagnosis than nonseminomatous germ cell tumors (NSGCT), are generally less advanced, and are associated with better survival. In fact, stage I seminoma represents the paradigm of a curable malignancy, with survival of 100% an expected outcome no matter what treatment option is chosen. However, consensus has not been reached among urologists and oncologists regarding the postoperative management of men with clinical stage I testicular seminoma.[3]
Currently, men are offered active surveillance, adjuvant radiation therapy, or single-agent chemotherapy (Table 1).[4] We will outline the treatment options for clinical stage I seminoma and discuss the controversies surrounding each approach.
Background and Risk-Adapted Strategies
TABLE 1


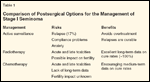
Comparison of Postsurgical Options for the Management of Stage I Seminoma
Over time, radiotherapy has established itself as an appropriate adjuvant treatment for clinical stage I seminoma, which significantly reduces the relapse rate.[5-9] Unfortunately, radiotherapy is associated with a doubling in the risk of developing a second malignancy compared with the general population; although absolute risks remain small.[10-14] Chemotherapy is probably equivalent to radiotherapy in terms of efficacy,[15] but long-term risks are unknown.[16] Active surveillance avoids overtreatment in the vast majority of patients, as only approximately 17% of patients are likely to relapse.[17] Therefore, recommendations for the treatment of clinical stage I seminoma have recently been updated.
The overriding theme of recent guidelines is the recognition that the options of surveillance, chemotherapy, and radiotherapy are all appropriate in the treatment of patients with clinical stage I seminoma.[4,18,19] Nevertheless, there are some caveats. For example, in the 2009 National Comprehensive Cancer Network (NCCN) Testicular Cancer Clinical Practice Guidelines, each of these options is rated category 1-that is, there is a uniform consensus among experts regarding their recommendation as approved treatment. In the fine print, however, surveillance is recommended as category 1 only for patients who have undergone previous radiotherapy, who have a horseshoe kidney, or who have inflammatory bowel disease. Surveillance is considered category 2B for others motivated to undergo follow-up and more intensive imaging. Meanwhile, chemotherapy has been raised to equal status with the more traditionally used radiotherapy as NCCN category 1 for all comers. This is despite long-term toxicity data and is based on early data demonstrating equivalent short-term efficacy with radiotherapy, with very few side effects.[15] Medical oncologists believe that along with its demonstrated efficacy, chemotherapy is less burdensome and toxic than radiotherapy, requires minimal hospital contact, reduces anxiety, and results in few reported relapses at just under 10 years’ follow-up. Moreover, salvage chemotherapy remains a viable option even if relapse occurs.[20-22]

The most recent European Association of Urology (EAU) guidelines offer similar preferences, with surveillance as a grade B recommendation behind chemotherapy and radiotherapy (category A).[19]
Participants in the more recent European Consensus Conference on Diagnosis and Treatment of Germ Cell Cancer stated that all three treatment options-surveillance, adjuvant carboplatin, and adjuvant radiotherapy-are acceptable strategies for the management of patients with clinical stage I seminoma.[18] With such an approach, those at higher risk of relapse may be offered surveillance with more confidence. Those patients without risk factors for recurrence may be more likely to be offered adjuvant radiotherapy or chemotherapy. A significant proportion of patients may therefore avoid overtreatment. Risk stratification was based on the original work of Warde et al,[9] who identified rete testis invasion and size of primary tumor (> 4 cm) as risk factors for relapse in a pooled analysis of surveillance studies with 638 patients. The relapse rate was 17% for primary tumors > 4 cm without rete testis invasion, 12% for primary tumor < 4 cm and no rete testis invasion, and 14% for rete testis invasion and a primary tumor < 4 cm. The difficulty is that such strategies have not been supported in prospective cohorts. Whatever the approach, high-risk patients treated with adjuvant chemotherapy or radiation therapy still have a 3% to 4% relapse rate.[20] Possible susceptibility of germ cell tumor patients to other diseases is generally attributed to the late treatment effects of radiation (such as cardiotoxicity) or a second malignancy, thus contributing to a decreased survival compared with matched individuals in the general population.[24]
Active Surveillance
In a recent meta-analysis, the relapse rate for patients undergoing active surveillance was 17%, with disease-specific survival close to 100%.[17] Such data are compelling when considering active surveillance as an option. The benefits are clear: avoidance of overtreatment in over 80% of patients; knowledge that relapses are salvageable; no risk to fertility; no risk of acute toxicity, and no iatrogenic risk of cardiotoxicty or second malignancy. Against this, surveillance does oblige the patient to close follow-up and vigorous imaging; even in a study situation, this is not always achieveable.[25] Anxiety is also a potential effect of surveillance,[26] and this is where selection of patients who accept the risk of relapse is essential.
Radiotherapy
The efficacy of radiotherapy in treating clinical stage I seminoma has been reported in numerous series, with a 5-year progression-free survival of over 95% and nearly all relapses occurring outside the radiation field.[27] Short-term toxicities are usually mild, with nausea and vomiting, diarrhea, fatigue, and skin erythema being the most common.[28] However, the long-term cost to patients is only now being fully understood. The risk of a second malignancy doubles in these patients, compared with the general population. The risk of a solid cancer is between 5% and 10%, and the absolute risk is about twice that seen in the general population. This translates into an additional six to nine cancers over the 25 years after treatment for every 100 men treated. These malignancies are usually confined to the area of irradiation such as the bladder, kidney, skin, and stomach, but prostate, lung, and head and neck cancers have been reported outside those fields, likely secondatry to radiation scatter.[10-14,29]
Furthermore, radiotherapy is associated with cardiotoxicity in the long term, also due to radiation scatter and not direct damage, because irradiated areas are below the diaphragm.[24,30] Both factors contribute to a decreased survival compared to other men in the general population.[24]
In recognition of these effects, radiotherapy fields have been modified from the pre-1990 model of anteriorly and posteriorly delivered so called “dogleg” fields that covered lymphatic drainage of the testis to include the ipsilateral pelvis and the para-aortic region. This has not resulted in a reduction in survival rates, but isolated cases of recurrence at the edge of traditional fields have been surfacing in the literature.[28,31-34] The reduction of overall treatment doses is also being explored but reductions beyond 30 and 20 Gy have yet to be published. Any reduction in overall dose is thought to reduce the late radiation effects,[23] as is reducing the daily dose fraction from 2 to 1.5 Gy.[35] Risks to fertility remain despite shielding of the contralateral testis. They may be related to the disease process itself, and not just the treatment.[23,36]
Chemotherapy
Case Report: A Young Man With a Testicular Mass
An otherwise healthy 26-year-old male university student presented with a 2-cm mass in his right testicle. The tumor is confirmed as solid on ultrasound. Tumor markers are negative and staging computed tomography and chest radiography reveal no evidence of metastatic disease.
An orchiectomy is undertaken, with final pathology demonstrating pure classical seminoma without rete testis involvement. The patient is not married but wishes to have children in the future. Should he have adjuvant treatment or undergo active surveillance?
The patient is level-headed and receptive to compliance issues. However, his case is complicated by the fact that he may move to a new city after graduating from college. Certainly active surveillance must be discussed, but we are also conscious of the imaging and surveillance burden, combined with the fact that this patient may move away and require treatment at a different center. After being given all three options, he chooses active surveillance. Despite moving to a new city, he continues with imaging and follow-up and remains disease-free at 3 years.
If the patient were unreliable and poorly motivated, surveillance would not have been the best option. Clearly, radiotherapy or chemotherapy could also have been undertaken, but in our center, prior to these treatments he would need to undergo sperm-banking. Furthermore, the risks of cardiotoxicity and second malignancy with radiation are genuine concerns. Nevertheless, in the case of a more unreliable patient, radiotherapy would be the preferred treatment option due to the lack of long-term toxicity data for chemotherapy.
The rationale for chemotherapy was borne out of concern with the secondary effects of radiotherapy as well as with the recognition that where tumors are sensitive to chemotherapy, reduced doses have often been successful. Carboplatin has emerged as a primary adjuvant treatment alternative for stage I seminoma based on the use of combination chemotherapy for higher-stage germ cell tumors. The short-term toxicities from single- or dual-dose chemotherapy for seminoma are minimal but include gastrointestinal side effects and fatigue. In the long term, data are unknown and hypothetical, but based on longer-duration courses of chemotherapy for nonseminomatous tumors, the possibilities of cerebrovascular disease, infertility, neuropathy, and leukemia as well as other second malignancies remain. Cardiotoxicity may not be a concern.[22,29,37]
Although the most recent publication concerning a single cycle of carboplatin included only a modest follow-up of 4 years, it proved to be noninferior to radiotherapy in terms of relapse rates and survival.[15] Despite this evidence and guideline recommendations as outlined previously, many authors believe that carboplatin should not be considered the standard of care.[37,38] Others have argued that two courses of treatment are necessary when carboplatin is used.[20,21] Even with two cycles, a small but significant percentage of patients (3%–4%) experience a recurrence in the retroperitoneum.
Discussion


Stage I seminoma is a highly curable disease but does require some degree of follow-up. The aim of follow-up of testicular cancer patients is twofold: (1) to detect relapses early when minimal disease is present so that they may be salvaged, and (2) to detect and manage the effects of the original definitive oncologic treatment.
A major criticism of active surveillance is that the required number of follow-up investigations brings on anxiety that reduces quality of life. In addition, the multiple follow-up visits increase health-care costs. That said, it is worth noting that the 2009 NCCN guidelines[4] recommend the same imaging and follow-up whether a man is treated with surveillance or chemotherapy. Among men who have undergone radiation therapy, imaging of the retroperitoneum is not required due to the reduced risk of recurrence.
Similar to the treatment paradigm, a non–evidence-based, risk-adapted follow-up strategy has been recommended.[39,40] Studies are currently underway to reduce the use of computed tomography in surveillance of testicular tumors such that more limited protocols may be developed, thus reducing potential risk of radiation.[41]
Quality-adjusted life-year (QALY) assessments show a similar result-around 20-for all three modalities, but the cost per QALY is greater for surveillance and similar for radiation and chemotherapy.[42] Surveillance regimens are likely to be reduced in the coming years, altering the cost of surveillance and leaving only toxicities and overtreatment as issues to consider.
In conclusion, we believe that if a patient is willing and able to comply with a surveillance policy, then long-term close follow-up should be recommended after orchiectomy for clinical stage I seminoma. This is because radiotherapy and chemotherapy will overtreat > 80% of patients, with the possibility of acute and late toxicities, while surveillance patients have the same ultimate cure rate. Long-term data on survival and toxicities of chemotherapy are not yet available for large numbers of patients. However, each center must factor in staff experience, costs, compliance, psychosocial issues, and the impact on fertility for any individual patient prior to selecting a treatment.
The future may yield risk-adapted strategies not only for providing details on prognosis and giving information for selecting the appropriate adjuvant treatment, but also to help minimize follow-up in surveillance patients and reduce costs to the community.
Financial Disclosure: The authors have no significant financial interest or other relationship with the manufacturers of any products or providers of any service mentioned in this article.
References:
1. Steele GS, Richie JP, Stewart AK, et al: The National Cancer Data Base report on patterns of care for testicular carcinoma, 1985-1996. Cancer 86:2171-2183, 1999.
2. Jemal A, Siegel R, Ward E, et al: Cancer statistics, 2008. CA Cancer J Clin 58:71-96, 2008.
3. Fleshner N, Warde P: Controversies in the management of testicular seminoma. Semin Urol Oncol 20:227-233, 2002.
4. National Comprehensive Cancer Network: The NCCN testicular cancer clinical practice guidelines in oncology, vol 1, version 2. Available at www.nccn.org, Accessed June 19, 2009.
5. Bosl GL, Bajorin DF, Sheinfeld J, et al: Cancer of the testis, in Devita VT, Hellman S, Rosenberg SA (eds): Cancer: Principles and Practice of Oncology, 7th ed, pp 1269-1293. Philadelphia, Lippincott Williams & Wilkins, 2005.
6. Chung P, Parker C, Panzarella T, et al: Surveillance in stage I testicular seminoma-risk of late relapse. Can J Urol 9:1637-1640, 2002.
7. Gurkaynak M, Akyol F, Zorlu F, et al: Stage I testicular seminoma: Para-aortic and iliac irradiation with reduced dose after orchiectomy. Urol Int 71:385-388, 2003.
8. Garcia-Serra AM, Zlotecki RA, Morris CG, et al: Long-term results of radiotherapy for early-stage testicular seminoma. Am J Clin Oncol 28:119-124, 2005.
9. Warde P, Specht L, Horwich A, et al: Prognostic factors for relapse in stage I seminoma managed by surveillance: A pooled analysis. J Clin Oncol 20:4448-4452, 2002.
10. Bokemeyer C, Schmoll HJ: Secondary neoplasms following treatment of malignant germ cell tumors. J Clin Oncol 11:1703-1709, 1993.
11. Travis LB, Curtis RE, Storm H, et al: Risk of second malignant neoplasms among long-term survivors of testicular cancer. J Natl Cancer Inst 89:1429-1439, 1997.
12. Travis LB, Fosså SD, Schonfeld SJ, et al: Second cancers among 40,576 testicular cancer patients: Focus on long-term survivors. J Natl Cancer Inst 97:1354-1365, 2005.
13. Van Leeuwen FE, Stiggelbout AM, Van den Belt-Dusebout AW, et al: Second cancer risk following testicular cancer: A follow-up study of 1,909 patients. J Clin Oncol 11:415-424, 1993.
14. Wanderas EH, Fosså SD, Tretli S: Risk of subsequent non-germ cell cancer after treatment of germ cell cancer in 2006 Norwegian male patients. Eur J Cancer 33:253-262, 1997.
15. Oliver RTD, Mason MD, Mead GM, et al: Radiotherapy versus single-dose carboplatin in adjuvant treatment of stage I seminoma: A randomised trial. Lancet 366:293-300, 2005.
16. Loehrer PJ Sr, Bosl GJ: Carboplatin for stage I seminoma and the sword of Damocles. J Clin Oncol 23:8566-8569, 2005.
17. Groll RJ, Warde P, Jewett MA: A comprehensive systematic review of testicular germ cell tumor surveillance. Crit Rev Oncol Hematol 64:182-197, 2007.
18. Krege S, Beyer J, Souchon R, et al: European consensus conference on diagnosis and treatment of germ cell cancer: A report of the second meeting of the European Germ Cell Cancer Consensus group (EGCCCG): Part I. Eur Urol 53:478-496, 2008.
19. Albers P, Albrecht W, Algaba F, et al: Guidelines on testicular cancer. Arnhem, The Netherlands; European Association of Urology; 2008.
20. Dieckmann KP, Brüggeboes B, Pichlmeier U, et al: Adjuvant treatment of clinical stageâ¯I seminoma: Is a single course of carboplatin sufficient? Urology 55:102-106, 2000.
21. Oliver RTD, Edmonds PM, Ong JYH, et al: Pilot studies of 2 and 1 course carboplatin as adjuvant for stage I seminoma: Should it be tested in a randomized trial against radiotherapy? Int J Radiat Oncol Biol Phys 29:3-8, 1994.
22. Powles T, Robinson D, Shamash J, et al: The long-term risks of adjuvant carboplatin treatment for stage I seminoma of the testis. Ann Oncol 19:443-447, 2008.
23. Sava T, Consoli F, Santo A, et al: Adjuvant treatment in the management of testis-confined germ cell tumours after orchidectomy. BJU Int 101:155-159, 2008.
24. Zagars GK, Ballo MT, Lee AK, et al: Mortality after cure of testicular seminoma. J Clin Oncol 22:640-647, 2004.
25. Ernst DS, Brasher P, Venner PM, et al: Compliance and outcome of patients with stage 1 non-seminomatous germ cell tumors (NSGCT) managed with surveillance programs in seven Canadian centres. Can J Urol 12:2575-2580, 2005.
26. Moynihan C: Testicular cancer: The psychosocial problems of patients and their relatives. Cancer Surv 6:477-510, 1987.
27. Yang GY, Li B, Wagner TD, et al: Long-term outcome of stage I seminoma. Am J Clin Oncol 30:205-210, 2007.
28. Niewald M, Freyd J, Fleckenstein J, et al: Low-dose radiotherapy for stage I seminoma-long-term results. Int J Radiat Oncol Biol Phys 66:1112-1119, 2006.
29. Gilligan T, Oh WK, Kantoff PW: Carboplatin for stage I seminoma (letter). J Clin Oncol 24:2971-2972, 2006.
30. Huddart RA, Norman A, Shahidi M, et al: Cardiovascular disease as a long-term complication of treatment for testicular cancer. J Clin Oncol 21:1513-1523, 2003.
31. Jones RH, Vasey PA: Part I: Testicular cancer-management of early disease. Lancet Oncol 4:730-737, 2003.
32. Horwich A: Radiotherapy in stage I seminoma of the testis. J Clin Oncol 22:585-588, 2004.
33. Fossa SD, Aass N, Kaalhus O: Radiotherapy for testicular seminoma stage I: Treatment results and long-term post-irradiation morbidity in 365 patients. Int J Radiat Oncol Biol Phys 16:383-388, 1989.
34. Fatigante L, Ducci F, Campoccia S, et al: Long-term results in patients affected by testicular seminoma treated with radiotherapy: Risk of second malignancies. Tumori 91:144-150, 2005.
35. Martin J, Chung P, Warde P: Treatment options, prognostic factors and selection of treatment in stage I seminoma. Onkologie 29:592-598, 2006.
36. Raman JD, Nobert CF, Goldstein M: Increased incidence of testicular cancer in men presenting with infertility and abnormal semen analysis. J Urol 174:1819-1822, 2005.
37. Loehrer PJ Sr, Bosl GJ: Carboplatin for stage I seminoma and the sword of Damocles. J Clin Oncol 23:8566-8569, 2005.
38. Feldman DR, Bosl GJ: Treatment of stage I seminoma: Is it time to change your practice? J Hematol Oncol 1:22, 2008.
39. Martin JM, Panzarella T, Zwahlen DB, et al: Evidence-based guidelines for following stage 1 seminoma. Cancer 109:2248-2256, 2007.
40. Tarin TV, Sonn G, Shinghal R: Estimating the risk of cancer associated with imaging related radiation during surveillance for stage I testicular cancer using computerized tomography. J Urol 181:627-633, 2009.
41. Rustin GJ, Mead GM, Stenning SP, et al: Randomized trial of two or five computed tomography scans in the surveillance of patients with stage I nonseminomatous germ cell tumors of the testis: Medical research council trial TE08, ISRCTN56475197 - The National Cancer Research Institute Testis Cancer Clinical Studies Group. J Clin Oncol 25:1310-1315, 2007.
42. Patrice SJ, Patrice JR, Steinberg JS, et al: A cost-effectiveness analysis of surveillance, radiotherapy, and carboplatin in the management of stage I testicular seminoma (abstract 6108). J Clin Oncol 24(18S):327s, 2006.
















